Readiness For Enhanced Knowledge N Fdar 3x931
This document was ed by and they confirmed that they have the permission to share it. If you are author or own the copyright of this book, please report to us by using this report form. Report 2z6p3t
Overview 5o1f4z
& View Readiness For Enhanced Knowledge N Fdar as PDF for free.
More details 6z3438
- Words: 535
- Pages: 4
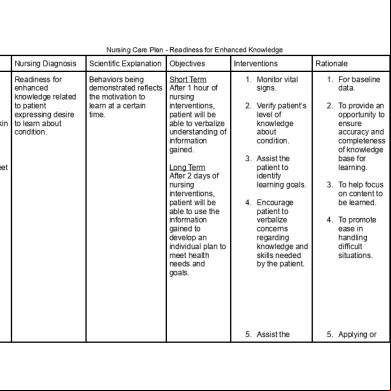
Nursing Care Plan - Readiness for Enhanced Knowledge
Assessment
Nursing Diagnosis
Scientific Explanation
Objectives
Readiness for enhanced “Ano po yung knowledge related eclampsia?” to patient expressing desire “Ano yung bawal sa akin to learn about niyan tsaka kailangan condition. ko gawin?”
Behaviors being demonstrated reflects the motivation to learn at a certain time.
Short Term After 1 hour of nursing interventions, patient will be able to verbalize understanding of information gained.
Subjective:
Objective: ● Edema of the feet ● VS taken as follows: ○ T: 36.5C ○ P: 98 ○ R: 19 ○ BP: 120/70
Long Term After 2 days of nursing interventions, patient will be able to use the information gained to develop an individual plan to meet health needs and goals.
Interventions
Rationale
1. Monitor vital signs.
1. For baseline data.
2. patient’s level of knowledge about condition.
2. To provide an opportunity to ensure accuracy and completeness of knowledge base for learning.
3. Assist the patient to identify learning goals. 4. Encourage patient to verbalize concerns regarding knowledge and skills needed by the patient.
5. Assist the
3. To help focus on content to be learned. 4. To promote ease in handling difficult situations.
5. Applying or
Expected Outcome Short Term The patient shall have verbalized understanding of the information gained. Long Term The patient shall have used the information gained to develop an individual plan to meet health needs and goals.
patient in identifying ways to use the information. 6. Repeat instructions and demonstrations of skills needed by the patient. 7. Encourage patient to ask questions and clarify information concerning condition.
using information increases the desire to learn and retain information. 6. Repetition reinforces learning. 7. To ensure complete knowledge concerning condition to prevent risks.
Date
Time
7/20/17
8:00 AM
Focus
Nurse’s Progress Notes
Readiness for enhanced knowledge as evidenced by patient expressing desire to learn about condition.
Data: Received patient on bed in sitting position, conscious and coherent. Patient had no contraptions and no complaints of pain. Patient verbalized “Ano po yung eclampsia?” and “Ano yung bawal sa akin niyan tsaka kailangan ko gawin?” Presence of edema on feet. Breasts- Breastfeeds effectively on both breasts. No tenderness or swelling. Uterus- Contracted 1 finger breadth below umbilicus. Bladder- Urinated 4 times, light yellow. Bowel- Defecated 1 time, semi-solid. Lochia- Lochia serosa. Pink color. Started using napkins the day after delivery. Changed napkin twice. Episiorrhaphy- Median, no swelling. Skin- Warm to touch. Good skin turgor. Homan’s Sign- Negative. Emotion- Patient is in the taking hold phase as evidenced by breastfeeding her baby. VS- T=36.5 C, P=98, R=19, BP=120/70 mmHg. Actions: Established rapport, provided AM care, stretched bed linens, monitored VS. Asked patient about previous VS and medications being taken. Assessed skin color and other extremities. Encouraged patient to eat fruits and vegetables. Encouraged patient to elevate legs when possible. Encouraged patient to drink water, buko juice, or pineapple juice to promote urination and defecation. Encouraged walking and exercising to promote venous return. Recommended ankle and foot exercises to reduce pooling. Discussed factors that affect circulation. Discouraged prolonged standing, tight clothing. Emphasized at-home BP monitoring. Response: After 1 hour of nursing interventions, patient will be able to verbalize understanding of information gained.
Assessment
Nursing Diagnosis
Scientific Explanation
Objectives
Readiness for enhanced “Ano po yung knowledge related eclampsia?” to patient expressing desire “Ano yung bawal sa akin to learn about niyan tsaka kailangan condition. ko gawin?”
Behaviors being demonstrated reflects the motivation to learn at a certain time.
Short Term After 1 hour of nursing interventions, patient will be able to verbalize understanding of information gained.
Subjective:
Objective: ● Edema of the feet ● VS taken as follows: ○ T: 36.5C ○ P: 98 ○ R: 19 ○ BP: 120/70
Long Term After 2 days of nursing interventions, patient will be able to use the information gained to develop an individual plan to meet health needs and goals.
Interventions
Rationale
1. Monitor vital signs.
1. For baseline data.
2. patient’s level of knowledge about condition.
2. To provide an opportunity to ensure accuracy and completeness of knowledge base for learning.
3. Assist the patient to identify learning goals. 4. Encourage patient to verbalize concerns regarding knowledge and skills needed by the patient.
5. Assist the
3. To help focus on content to be learned. 4. To promote ease in handling difficult situations.
5. Applying or
Expected Outcome Short Term The patient shall have verbalized understanding of the information gained. Long Term The patient shall have used the information gained to develop an individual plan to meet health needs and goals.
patient in identifying ways to use the information. 6. Repeat instructions and demonstrations of skills needed by the patient. 7. Encourage patient to ask questions and clarify information concerning condition.
using information increases the desire to learn and retain information. 6. Repetition reinforces learning. 7. To ensure complete knowledge concerning condition to prevent risks.
Date
Time
7/20/17
8:00 AM
Focus
Nurse’s Progress Notes
Readiness for enhanced knowledge as evidenced by patient expressing desire to learn about condition.
Data: Received patient on bed in sitting position, conscious and coherent. Patient had no contraptions and no complaints of pain. Patient verbalized “Ano po yung eclampsia?” and “Ano yung bawal sa akin niyan tsaka kailangan ko gawin?” Presence of edema on feet. Breasts- Breastfeeds effectively on both breasts. No tenderness or swelling. Uterus- Contracted 1 finger breadth below umbilicus. Bladder- Urinated 4 times, light yellow. Bowel- Defecated 1 time, semi-solid. Lochia- Lochia serosa. Pink color. Started using napkins the day after delivery. Changed napkin twice. Episiorrhaphy- Median, no swelling. Skin- Warm to touch. Good skin turgor. Homan’s Sign- Negative. Emotion- Patient is in the taking hold phase as evidenced by breastfeeding her baby. VS- T=36.5 C, P=98, R=19, BP=120/70 mmHg. Actions: Established rapport, provided AM care, stretched bed linens, monitored VS. Asked patient about previous VS and medications being taken. Assessed skin color and other extremities. Encouraged patient to eat fruits and vegetables. Encouraged patient to elevate legs when possible. Encouraged patient to drink water, buko juice, or pineapple juice to promote urination and defecation. Encouraged walking and exercising to promote venous return. Recommended ankle and foot exercises to reduce pooling. Discussed factors that affect circulation. Discouraged prolonged standing, tight clothing. Emphasized at-home BP monitoring. Response: After 1 hour of nursing interventions, patient will be able to verbalize understanding of information gained.
Related Documents c2h70
Readiness For Enhanced Knowledge N Fdar 3x931
October 2019 1,244
Readiness For Enhanced Knowledge Health 41p6x
October 2019 349
Readiness For Enhanced Hope N 3r5d2h
December 2021 0
Nursing Care Plan For Readiness For Enhanced Sleep N 6v3w3h
November 2019 283
Nursing Care Plan For Readiness For Enhanced Hope N 2c6d27
October 2019 186
Nursing Diagnosis-readiness For Enhanced Immunization Status 6fj2x
October 2019 553More Documents from "Raidis Pangilinan" 6u6yx

Fam Nursing Care Plan 1a3x4q
December 2019 96
Readiness For Enhanced Knowledge N Fdar 3x931
October 2019 1,244
Digest Of Ordillo V. Comelec (g.r. No. 93054) 3e2z2i
April 2020 29
Digest Of Eastern Shipping Lines, Inc. V. Ca (g.r. No. 97412) u4u6y
April 2020 26
Historical Development Of Criminology.docx 5t503w
December 2019 69