Contraction For The Latissimus Dorsi Using Surface Electromyography 4n4l4b
This document was ed by and they confirmed that they have the permission to share it. If you are author or own the copyright of this book, please report to us by using this report form. Report 2z6p3t
Overview 5o1f4z
& View Contraction For The Latissimus Dorsi Using Surface Electromyography as PDF for free.
More details 6z3438
- Words: 4,015
- Pages: 5
Journal of Electromyography and Kinesiology xxx (2013) xxx–xxx
Contents lists available at SciVerse ScienceDirect
Journal of Electromyography and Kinesiology journal homepage: www.elsevier.com/locate/jelekin
Comparison of exercises inducing maximum voluntary isometric contraction for the latissimus dorsi using surface electromyography Se-yeon Park a, Won-gyu Yoo b,⇑ a b
Department of Physical Therapy, The Graduate School, Inje University, Republic of Korea Department of Physical Therapy, College of Biomedical Science and Engineering, Inje University, 607 Obangdong, Gimhae, Gyeongsangnam-do 621-749, Republic of Korea
a r t i c l e
i n f o
Article history: Received 8 February 2013 Received in revised form 15 April 2013 Accepted 19 May 2013 Available online xxxx Keywords: Electromyography Latissimus dorsi Selective activation
a b s t r a c t The aim of this study was to compare muscular activation during five different normalization techniques that induced maximal isometric contraction of the latissimus dorsi. Sixteen healthy men participated in the study. Each participant performed three repetitions each of five types of isometric exertion: (1) conventional shoulder extension in the prone position, (2) caudal shoulder depression in the prone position, (3) body lifting with shoulder depression in the seated position, (4) trunk bending to the right in the lateral decubitus position, and (5) downward bar pulling in the seated position. In most participants, maximal activation of the latissimus dorsi was observed during conventional shoulder extension in the prone position; the percentage of maximal voluntary contraction was significantly greater for this exercise than for all other normalization techniques except downward bar pulling in the seated position. Although differences in electrode placement among various electromyographic studies represent a limitation, normalization techniques for the latissimus dorsi are recommended to minimize error in assessing maximal muscular activation of the latissimus dorsi through the combined use of shoulder extension in the prone position and downward pulling. Ó 2013 Elsevier Ltd. All rights reserved.
1. Introduction In most electromyographic (EMG) studies, EMG normalization is performed by expressing the EMG amplitude relative to that of a maximal or submaximal voluntary contraction (Burden, 2010). Normalized EMG activity is used to compare activity levels among subjects and exercises. Without the use of an appropriate normalization method, however, EMG amplitude values may exceed 100% maximal voluntary contraction (MVC), despite the ‘‘maximal’’ nature of this measurement (Youdas et al., 2010; Hautier et al., 2000). The use of different normalization methods and electrode placement sites has limited the comparability of previous findings. Although some studies have established normalization techniques for specific muscles, research on this is lacking, so that electromyography (EMG) and manual muscle tests are generally used (Kendall et al., 2005; Hislop and Montgomery, 2002; Cram et al., 1998). Several studies have sought to identify appropriate normalization methods for muscles of the upper extremity (Boettcher et al., 2008; Ekstrom et al., 2005; Smith et al., 2004). Ekstrom et al. (2005) compared various normalization methods for the serratus anterior and upper and lower trapezius muscles, and Smith et al. (2004) investigated rhomboid muscle EMG activity during ⇑ Corresponding author. Tel.: +82 55 320 3994; fax: +82 55 329 1678.
three different manual muscle tests. Although these two studies identified appropriate normalization methods for the scapulothoracic musculature, no similar finding has been reported for other muscles, such as the latissimus dorsi (LD). To our knowledge, only two studies have investigated normalization methods for the latissimus dorsi (LD) using specific shoulder and trunk movements (Vera-Garcia et al., 2010; Boettcher et al., 2008). Vera-Garcia et al. (2010) compared 11 maximum voluntary contraction (MVC) techniques for the trunk musculature in healthy young females, but they excluded movements such as shoulder extension and depression, which are also important components of shoulder movement. Boettcher et al. (2008) investigated standard MVC techniques for shoulder muscles, including the LD, but excluded trunk bending movements. Although both studies found an appropriate MVC method related to specific trunk and shoulder movements and provided useful recommendations for researchers, normalization techniques for the LD still need to be investigated, due to its characteristics. The LD is a very broad muscle that arises from the lower six thoracic vertebrae, lumbodorsal fascia, sacrum, and iliac ala; along with the teres major, it inserts on the medial edge of the bicipital sulcus of the humerus (Cram et al., 1998). This muscle contributes to shoulder adduction, internal rotation, and extension, and it directly connects the upper extremity and trunk. Because of its importance, researchers have investigated several exercise meth-
E-mail address: [email protected] (W.-g. Yoo). 1050-6411/$ - see front matter Ó 2013 Elsevier Ltd. All rights reserved. http://dx.doi.org/10.1016/j.jelekin.2013.05.003
Please cite this article in press as: Park S-y, Yoo W-g. Comparison of exercises inducing maximum voluntary isometric contraction for the latissimus dorsi using surface electromyography. J Electromyogr Kinesiol (2013), http://dx.doi.org/10.1016/j.jelekin.2013.05.003
2
S.-y. Park, W.-g. Yoo / Journal of Electromyography and Kinesiology xxx (2013) xxx–xxx
ods and instruments to activate the LD (Youdas et al., 2010; Koyama et al., 2010; Snyder and Leech, 2009; Lehman et al., 2004). However, the use of different normalization methods in assessments of the same exercises has limited the ability to interpret results. For instance, for a lat pull-down (LPD) exercise using the same load, Koyama et al. (2010) investigated the effects of freedom of movement on LD activation and reported almost 50% MVC, whereas Snyder and Leech (2009) reported almost 70% MVC. Various methods of determining the MVC of the LD have been used for healthy and diseased individuals (Hislop and Montgomery, 2002; Kendall et al., 2005; Signorile et al., 2002). Shoulder extension in the prone position (EP) is a widely used manual muscle test (Hislop and Montgomery, 2002; Kendall et al., 2005). Prone shoulder depression and body lifting in the seated position (BL) have been used to independently activate the LD (Hislop and Montgomery, 2002). Lateral bending of the upper trunk in the lateral decubitus position (UTB) has also been recommended (VeraGarcia et al., 2010). Most recent studies have used isometric pulldown exertion with the shoulder abducted to 90° and the elbow flexed to 90° (Snyder and Leech, 2009; Lehman et al., 2004). No previous study has compared these methods for the normalization of LD activity. Therefore, the main purpose of this study was to assess the LD muscle activity in five exercise positions used to measure the MVC by EMG. A secondary purpose was to determine an appropriate normalization method from these five MVC positions for LD muscle assessment.
2. Materials and methods 2.1. Subjects Sixteen males were recruited from the local university using convenience sampling. For participant homogeneity, healthy right-arm dominant males with a body mass index (BMI) 625 were included in this study. Subjects with a history of upper- or lowerextremity injury within 6 months were excluded. Before conducting the experiments, a pilot study was performed to identify any limitation in the range of motion of the upper extremity and shortness of the latissimus dorsi. Participants ranged from 21 to 24 years of age, mean height was 178.1 ± 5.6 cm, mean weight was 69.6 ± 8.5 kg, and the mean BMI was 21.8 ± 1.8 kg/m2. The ethics committee of the University of Inje approved this study, and all volunteers gave written informed consent before participation.
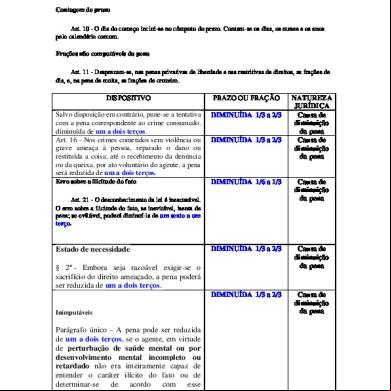
2.2. Electromyography A Trigno wireless system (Delsys, Boston, MA, USA) was used to obtain EMG signals. A single-channel surface electrode was placed at an oblique angle (25°) over the LD muscle on the dominant (right) side, approximately 4 cm below the inferior tip of the scapula and midway between the spine and lateral edge of the torso (Cram et al., 1998). The electrode was placed on the abdominal muscle site after inducing shoulder adduction, extension, and internal rotation in a seated position. Although one researcher placed the electrodes on all participants, the sites used differed among participants due to adduction, extension, and internal rotation. We placed the electrodes on abdominal muscle sites adjacent to those confirmed by geometric measurements. The skin site was initially prepared by shaving and abrasion, followed by cleaning with an alcohol swab to reduce impedance. The Trigno electrode used in this study has a band of 20–450 Hz and a commonmode rejection ratio of 80 dB. The researchers controlled data acquisition and processing on a laptop computer using EMGWorks software (Delsys Boston, MA, USA). Data were collected at a sampling rate of 2000 Hz and processed at 0.125-s intervals using the root mean square method. 2.3. Experimental procedures Resting EMG activity was recorded while the subject lay in a relaxed prone position. The participant was then asked to perform three trials of five isometric exertions believed to effectively activate the LD. Prior to testing, the participant was given 1 min of practice time for each exercise set. All exercises were performed for 5 s against manually applied resistance while the data were recorded, with a minimum 30-s rest between contractions. The participants rested for 5 min between exercise sessions. The order of exercise execution was randomized among participants. The five isometric exertions are described below (Fig. 1). (1) EP (Kendall et al., 2005; Hislop and Montgomery, 2002; Youdas et al., 2010): the participant lay prone on a bench with his arms by his sides and the shoulders internally rotated to create a palm-up position. From this position, the participant tried to move his shoulder toward the ceiling (extension). Downward manual resistance was applied to the forearm, and pressure was exerted on the contralateral side of the pelvis.
Fig. 1. The five exercises aimed at maximally activating the latissimus dorsi muscle. (1) Extension in Prone (EP), (2) caudal depression (CD), (3) body lifting (BL), (4) upper trunk bending (UTB), (5) Lat pull down (LPD).
Please cite this article in press as: Park S-y, Yoo W-g. Comparison of exercises inducing maximum voluntary isometric contraction for the latissimus dorsi using surface electromyography. J Electromyogr Kinesiol (2013), http://dx.doi.org/10.1016/j.jelekin.2013.05.003
3
S.-y. Park, W.-g. Yoo / Journal of Electromyography and Kinesiology xxx (2013) xxx–xxx
(2) Caudal depression (CD) (Hislop and Montgomery, 2002; Hughes and McBride, 2005): the participant lay prone on a bench with his arms by his sides and the shoulders internally rotated to create a palm-up position. He grasped handles located beside the bench and raised the right shoulder to chin level. The subject then tried to depress the right arm caudally while keeping the trunk (rib cage to pelvis) against the fixed handle. (3) BL (Hislop and Montgomery, 2002): the participant sat with his hands placed flat on tables located adjacent to the hips. Push-up handles and plates under the buttocks were used to ensure that the subject remained seated without flexing the elbow or depressing the shoulder. The subject then tried to depress his arms caudally and lift his body. Downward manual resistance was applied to the pelvis to prevent further elevation of the body. (4) Right and left UTB (Vera-Garcia et al., 2010): the participant attempted to bend the upper trunk laterally in the frontal plane while in the lateral decubitus position with the knees bent. The knees were secured with a belt, and the thorax and arms were braced manually by the researcher. (5) LPD (Snyder and Leech, 2009; Lehman et al., 2004; Signorile et al., 2002): in a seated position, the participant grasped a fixed crossbar using a wide grip with the elbows flexed to 90°. The participant was then asked to pull down on the bar as if attempting to break it. A researcher stabilized the participant by pressing downward on the shoulders to ensure that the contraction was isometric. The EMG values of the three trials were averaged. Of the five MVC techniques for the LD, the highest mean value was used to normalize the procedure (Vera-Garcia et al., 2010; Ekstrom et al., 2005 The intra-class correlation coefficient [ICC (3,1)] was P0.75 for each technique, which is regarded as good reliability (Fleiss, 1986). For statistical analyses, EMG data were expressed as a percentage of maximum EMG amplitude produced and referred to as the percentage of MVC (%MVC).
2.4. Statistical analysis The SPSS statistical package (version 18.0; SPSS, Inc., Chicago, IL, USA) was used to analyze differences in LD activation during the five normalization techniques. As a within-factor design, oneway repeated-measures analysis of variance was conducted to evaluate the differences in the% relative RMS–EMG among the five isometric MVC exercises. When necessary, post hoc Bonferroni corrections were performed to identify differences among the five exercises. All significance levels were set at P < 0.05. 3. Results Normalized EMG data for the LD differed significantly among normalization techniques. LD activation was increased significantly during EP compared with CD, BL, and UTB (P < 0.05; Fig. 2). The average%MVC was 92.62 ± 15.1 (95% confidence interval (CI) 85.57–100.69) in EP, 43.14 ± 19.23 (95% CI 32.88–53.39) in CD, 61.42 ± 27.38 (95% CI 46.83–76.02) in LB, 34.8 ± 15.36 (95% CI 26.62–42.99) in UTB, and 69.68 ± 30.49 (95% CI 53.43– 85.92) in LPD. The LPD resulted in significantly greater LD activation than did UTB (P 6 0.05; Fig. 2). Table 1 compares the%MVC values among the normalization techniques. 4. Discussion In the present study, we examined the EMG activity of the LD during five different normalization techniques. Research in kinesiology has demonstrated that this muscle contributes to shoulder extension, depression, adduction, and internal rotation, as well as trunk bending (Kendall et al., 2005; Hislop and Montgomery, 2002). The normalization techniques included in the present study induce at least some of these actions. Although previous clinical studies have used some or all of these techniques, differences among techniques have not been examined statistically. In the present study, LD activation was greatest during EP (8/16 partici-
Fig. 2. The normalized sEMG data (%MVC, mean ± SD) of the latissimus dorsi during the 5 different normalization techniques. ⁄Significant difference between techniques.
Table 1 Comparison of 5 different exercises using pair-wise comparison, mean differences and 95% confidence intervals (%MVC). Muscles
Exercises
Mean difference (95% CI) Extension prone
Latissimus dorsi
*
Caudal depression Lifting body Upper trunk bending Lat pull down
49.48* ( 31.19* ( 57.81* ( 22.94 (
67.03 31.93) 54.59 7.78) 73.57 42.05) 54.96 9.08)
Caudal depression
Lifting body
Upper trunk bending
– 18.28 ( 10.68 47.26) 8.33 ( 27.19 10.52) 26.54 ( 2.27 55.35)
– –
– – – 34.87* (4.91 64.83)
26.62 ( 46.08 7.15) 8.25 ( 21.01 37.52)
Significant difference between conditions.
Please cite this article in press as: Park S-y, Yoo W-g. Comparison of exercises inducing maximum voluntary isometric contraction for the latissimus dorsi using surface electromyography. J Electromyogr Kinesiol (2013), http://dx.doi.org/10.1016/j.jelekin.2013.05.003
4
S.-y. Park, W.-g. Yoo / Journal of Electromyography and Kinesiology xxx (2013) xxx–xxx
pants) or LPD (7/16 participants); in one participant, it was greatest during BL. Although no significant difference was observed between the EP and LPD techniques, the LPD data exhibited a lower average%MVC and greater variability (SD = 30.49) than the EP (SD = 15.1). When pulling the bar down with a flexed elbow and abducted shoulder, in addition to the LD and teres major, the posterior deltoid, biceps brachii, and pectoralis major could be recruited for shoulder adduction, elbow flexion, and scapular depression (Snyder and Leech, 2009, Sperandei et al., 2009). Large between-subject effects in the LPD may also have been present. Although we instructed the participants on how to perform the LPD and allowed them to practice, trained subjects might be able to alter their muscle activity voluntarily, emphasizing the LD (Snyder and Leech, 2009). The potential for recruiting a number of muscles during LPD exertion and differences among individuals might lead to large variability in the%MVC during LPD exertion. Our results demonstrated that LD activation was significantly greater during EP than during other exercises, except LPD. The mean difference between data obtained during EP and UTB and the calculation of MVC values >50% for EP and CD demonstrate that the inappropriate use of MVC can lead to the misinterpretation of exercise effects, such as the calculation of values representing >100% MVC or relatively higher%MVC values than obtained for other musculature. Three previous studies investigated the effects of pull-down exercises on LD activation (Koyama et al., 2010; Snyder and Leech, 2009; Signorile et al., 2002); two of these studies used the same EMG normalization method (LPD) and reported similar LD activation (70% MVC), whereas the third study (Koyama et al., 2010) used a similar exercise load but a different normalization technique (shoulder extension in the seated position, similar to EP) and reported an MVC of 50%. The only difference between the former two studies and the latter study was the normalization technique. We speculate that shoulder extension activates more LD muscle during the LPD than does shoulder adduction. The greater LD activation during MVC using shoulder extension reported in the third study compared with the first two studies is similar to our findings. Although we found no significant difference between EP and LPD, LD activation was greater in the EP than in the LPD, with a mean difference of 22% MVC. No participant showed maximal LD activation during CD or UTB. Although both of these exercises have been used to normalize EMG data for the LD (Vera-Garcia et al., 2010; Hughes and McBride, 2005), these results indicate that they induced less LD activation than did EP and LPD, with large mean differences. These differences between previous findings and our results may be due to differences in electrode placement on LD muscle sites rather than to errors in sEMG measurement. Previous studies of the trunk musculature during certain movements and postures described the sEMG site for the LD as ‘‘lateral to T9,’’ which is more medial and superior than the site used in the present study (Vera-Garcia et al., 2010; Drake et al., 2006). Paton and Brown (1995) suggested the possibility of functional differentiation within LD fibers, with caudal fibers of the LD preferentially activated in accordance with the direction of exertion at the shoulder t. This possibility means that movements such as UTB may activate other LD sites. Therefore, the%MVC results obtained in the present study may differ from those that would be obtained with the use of medial or superior LD sites. CD and BL, which are alternatives to EP, have been suggested to independently activate the LD muscle (Hislop and Montgomery, 2002). Both of these exercises aim to induce shoulder depression against resistance but result in less LD activation than do EP and LPD. Boettcher et al. (2008) recently demonstrated that normalization techniques for the LD involve internal rotation or extension of the shoulder t. Previous studies have not included shoulder
depression, preventing comparison with the present study, but our results suggest that CD might produce less accurate MVC values than do EP and LPD. Some limitations of this study should be considered. First, although the study compared normalization techniques for the LD muscle, it a small number of only male participants were included. Second, we used a single electrode site to measure the LD activity, whereas clinical studies generally use additional LD sites. Third, we could not record kinematic data throughout the experiment, preventing a numerical representation of the magnitudes of extension and internal rotation. Fourth, generalization to other populations, such as individuals with shoulder pathology, was not possible. Fifth, this study included only exercises that induce maximum voluntary isometric contraction, and any future study should include a submaximal task for the normalization procedure. 5. Conclusion This study compared normalization techniques for the LD with the aim of identifying an adequate method. We confirmed that EP, which is generally recommended in the clinical literature, resulted in more LD activation than did the other techniques. We also found that LPD is also effective for normalizing LD activation. Considering the muscle actions that occur during a pulling motion, the shoulder extension, adduction, and internal rotation components might be activated during performance of LD normalization techniques, causing error in the MVC calculation. Conflict of interest None declare Acknowledgement This research was ed by Basic Science Research Program through the National Research Foundation of Korea (NRF) funded by the Ministry of Education, Science and Technology (No. 2012R1A1B4001058). References Burden A. How should we normalize electromyograms obtained from healthy participants? What we have learned from over 25 years of research. J Electromyogr Kinesiol 2010;20(6):1023–35. Boettcher CE, Ginn KA, Cathers I. Standard maximum isometric voluntary contraction tests for normalizing shoulder muscle EMG. J Orthop Res 2008;26(12):1591–7. Cram JR, Kasman GS, Holtz J. Introduction to surface electromyography. 1st ed. Gaithersburg: Aspen; 1998. Drake JD, Fischer SL, Brown SH, Callaghan JP. Do exercise balls provide a training advantage for trunk extensor exercises? A biomechanical evaluation. J Manipulative Physiol Ther 2006;29(5):354–62. Ekstrom RA, Soderberg GL, Donatelli RA. Normalization procedures using maximum voluntary isometric contractions for the serratus anterior and trapezius muscles during surface EMG analysis. J Electromyogr Kinesiol 2005;15:418–28. Fleiss J. The design and analysis of clinical experiments. 1st ed. Canada: John Wiley and Sons; 1986. Hautier CA, Arsac LM, Deghdegh K, Souquet J, Belli A, Lacour JR. Influence of fatigue on EMG/force ratio and cocontraction in cycling. Med Sci Sports Exerc 2000;32(4):839–43. Hislop HJ, Montgomery J. Muscle testing and function. 7th ed. Philadelphia: WB Saunders; 2002. Hughes CJ, McBride A. The use of surface electromyography to determine muscle activation during isotonic and elastic resistance exercise for shoulder rehabilitation. Orthopaedic Practice 2005;17(2):18–23. Kendall FP, McCreary EK, Provance PG, Rodgers MM, Romani WA. Muscles: testing and function, with posture and pain. 5th ed. Baltimore, MD: Lippincott Williams & Wilkins; 2005. Koyama Y, Kobayashi H, Suzuki S, Enoka RM. Enhancing the weight training experience: a comparison of limb kinematics and EMG activity on three machines. Eur J Appl Physiol 2010;109(5):789–801.
Please cite this article in press as: Park S-y, Yoo W-g. Comparison of exercises inducing maximum voluntary isometric contraction for the latissimus dorsi using surface electromyography. J Electromyogr Kinesiol (2013), http://dx.doi.org/10.1016/j.jelekin.2013.05.003
S.-y. Park, W.-g. Yoo / Journal of Electromyography and Kinesiology xxx (2013) xxx–xxx Lehman GJ, Buchan DD, Lundy A, Myers N, Nalborczyk A. Variations in muscle activation levels during traditional latissimus dorsi weight training exercises: an experimental study. Dyn Med 2004;3(1):4. Paton ME, Brown JM. Functional differentiation within latissimus dorsi. Electromyogr Clin Neurophysiol 1995;35(5):301–9. Signorile JF, Zink AJ, Szwed SP. A comparative electromyographical investigation of muscle utilization patterns using various hand positions during the lat pulldown. J Strength Cond Res 2002;16(4):539–46. Smith J, Padgett DJ, Kaufman KR, Harrington SP, An KN, Irby SE. Rhomboid muscle electromyography activity during 3 different manual muscle tests. Arch Phys Med Rehabil 2004;85(6):987–92. Snyder BJ, Leech JR. Voluntary increase in latissimus dorsi muscle activity during the lat pull-down following expert instruction. J Strength Cond Res 2009;23(8):2204–9. Sperandei S, Barros MA, Silveira-Júnior PC, Oliveira CG. Electromyographic analysis of three different types of lat pull-down. J Strength Cond Res 2009;23(7):2033–8. Vera-Garcia FJ, Moreside JM, McGill SM. MVC techniques to normalize trunk muscle EMG in healthy women. J Electromyogr Kinesiol 2010;20(1):10–6. Youdas JW, Amundson CL, Cicero KS, Hahn JJ, Harezlak DT, Hollman JH. Surface electromyographic activation patterns and elbow t motion during a pull-up, chin-up, or perfect-pullup™ rotational exercise. J Strength Cond Res 2010;24(12):3404–14.
5
Won-gyu Yoo received the Ph.D. in Physical Therapy Treatments for Musculoskeletal Disorders from the Yonsei University, the Republic of Korea, in 2008. He was the acting head of the Department of Physical Therapy at Inje University in Gimhea, Gyeongsangnamdo, Republic of Korea. He is working as the main researcher of National Research Foundation of Korea for posture correction research of computer s. His research interests include biological signal processing, chronic muscle pain and dysfunction due to overuse, and medical device development for physical therapy interventions.
Se-yeon Park received his master of science in physical therapy at the Inje university in 2012 and now is a doctor of science student in physical therapy and rehabilitation sciences at Inje university. He is currently working as a researcher of National Research Foundation of Korea and a member of the Korean Physical Therapy Association. His research interests include musculoskeletal response in physical therapy interventions, and scapular dyskinesis.
Please cite this article in press as: Park S-y, Yoo W-g. Comparison of exercises inducing maximum voluntary isometric contraction for the latissimus dorsi using surface electromyography. J Electromyogr Kinesiol (2013), http://dx.doi.org/10.1016/j.jelekin.2013.05.003
Contents lists available at SciVerse ScienceDirect
Journal of Electromyography and Kinesiology journal homepage: www.elsevier.com/locate/jelekin
Comparison of exercises inducing maximum voluntary isometric contraction for the latissimus dorsi using surface electromyography Se-yeon Park a, Won-gyu Yoo b,⇑ a b
Department of Physical Therapy, The Graduate School, Inje University, Republic of Korea Department of Physical Therapy, College of Biomedical Science and Engineering, Inje University, 607 Obangdong, Gimhae, Gyeongsangnam-do 621-749, Republic of Korea
a r t i c l e
i n f o
Article history: Received 8 February 2013 Received in revised form 15 April 2013 Accepted 19 May 2013 Available online xxxx Keywords: Electromyography Latissimus dorsi Selective activation
a b s t r a c t The aim of this study was to compare muscular activation during five different normalization techniques that induced maximal isometric contraction of the latissimus dorsi. Sixteen healthy men participated in the study. Each participant performed three repetitions each of five types of isometric exertion: (1) conventional shoulder extension in the prone position, (2) caudal shoulder depression in the prone position, (3) body lifting with shoulder depression in the seated position, (4) trunk bending to the right in the lateral decubitus position, and (5) downward bar pulling in the seated position. In most participants, maximal activation of the latissimus dorsi was observed during conventional shoulder extension in the prone position; the percentage of maximal voluntary contraction was significantly greater for this exercise than for all other normalization techniques except downward bar pulling in the seated position. Although differences in electrode placement among various electromyographic studies represent a limitation, normalization techniques for the latissimus dorsi are recommended to minimize error in assessing maximal muscular activation of the latissimus dorsi through the combined use of shoulder extension in the prone position and downward pulling. Ó 2013 Elsevier Ltd. All rights reserved.
1. Introduction In most electromyographic (EMG) studies, EMG normalization is performed by expressing the EMG amplitude relative to that of a maximal or submaximal voluntary contraction (Burden, 2010). Normalized EMG activity is used to compare activity levels among subjects and exercises. Without the use of an appropriate normalization method, however, EMG amplitude values may exceed 100% maximal voluntary contraction (MVC), despite the ‘‘maximal’’ nature of this measurement (Youdas et al., 2010; Hautier et al., 2000). The use of different normalization methods and electrode placement sites has limited the comparability of previous findings. Although some studies have established normalization techniques for specific muscles, research on this is lacking, so that electromyography (EMG) and manual muscle tests are generally used (Kendall et al., 2005; Hislop and Montgomery, 2002; Cram et al., 1998). Several studies have sought to identify appropriate normalization methods for muscles of the upper extremity (Boettcher et al., 2008; Ekstrom et al., 2005; Smith et al., 2004). Ekstrom et al. (2005) compared various normalization methods for the serratus anterior and upper and lower trapezius muscles, and Smith et al. (2004) investigated rhomboid muscle EMG activity during ⇑ Corresponding author. Tel.: +82 55 320 3994; fax: +82 55 329 1678.
three different manual muscle tests. Although these two studies identified appropriate normalization methods for the scapulothoracic musculature, no similar finding has been reported for other muscles, such as the latissimus dorsi (LD). To our knowledge, only two studies have investigated normalization methods for the latissimus dorsi (LD) using specific shoulder and trunk movements (Vera-Garcia et al., 2010; Boettcher et al., 2008). Vera-Garcia et al. (2010) compared 11 maximum voluntary contraction (MVC) techniques for the trunk musculature in healthy young females, but they excluded movements such as shoulder extension and depression, which are also important components of shoulder movement. Boettcher et al. (2008) investigated standard MVC techniques for shoulder muscles, including the LD, but excluded trunk bending movements. Although both studies found an appropriate MVC method related to specific trunk and shoulder movements and provided useful recommendations for researchers, normalization techniques for the LD still need to be investigated, due to its characteristics. The LD is a very broad muscle that arises from the lower six thoracic vertebrae, lumbodorsal fascia, sacrum, and iliac ala; along with the teres major, it inserts on the medial edge of the bicipital sulcus of the humerus (Cram et al., 1998). This muscle contributes to shoulder adduction, internal rotation, and extension, and it directly connects the upper extremity and trunk. Because of its importance, researchers have investigated several exercise meth-
E-mail address: [email protected] (W.-g. Yoo). 1050-6411/$ - see front matter Ó 2013 Elsevier Ltd. All rights reserved. http://dx.doi.org/10.1016/j.jelekin.2013.05.003
Please cite this article in press as: Park S-y, Yoo W-g. Comparison of exercises inducing maximum voluntary isometric contraction for the latissimus dorsi using surface electromyography. J Electromyogr Kinesiol (2013), http://dx.doi.org/10.1016/j.jelekin.2013.05.003
2
S.-y. Park, W.-g. Yoo / Journal of Electromyography and Kinesiology xxx (2013) xxx–xxx
ods and instruments to activate the LD (Youdas et al., 2010; Koyama et al., 2010; Snyder and Leech, 2009; Lehman et al., 2004). However, the use of different normalization methods in assessments of the same exercises has limited the ability to interpret results. For instance, for a lat pull-down (LPD) exercise using the same load, Koyama et al. (2010) investigated the effects of freedom of movement on LD activation and reported almost 50% MVC, whereas Snyder and Leech (2009) reported almost 70% MVC. Various methods of determining the MVC of the LD have been used for healthy and diseased individuals (Hislop and Montgomery, 2002; Kendall et al., 2005; Signorile et al., 2002). Shoulder extension in the prone position (EP) is a widely used manual muscle test (Hislop and Montgomery, 2002; Kendall et al., 2005). Prone shoulder depression and body lifting in the seated position (BL) have been used to independently activate the LD (Hislop and Montgomery, 2002). Lateral bending of the upper trunk in the lateral decubitus position (UTB) has also been recommended (VeraGarcia et al., 2010). Most recent studies have used isometric pulldown exertion with the shoulder abducted to 90° and the elbow flexed to 90° (Snyder and Leech, 2009; Lehman et al., 2004). No previous study has compared these methods for the normalization of LD activity. Therefore, the main purpose of this study was to assess the LD muscle activity in five exercise positions used to measure the MVC by EMG. A secondary purpose was to determine an appropriate normalization method from these five MVC positions for LD muscle assessment.
2. Materials and methods 2.1. Subjects Sixteen males were recruited from the local university using convenience sampling. For participant homogeneity, healthy right-arm dominant males with a body mass index (BMI) 625 were included in this study. Subjects with a history of upper- or lowerextremity injury within 6 months were excluded. Before conducting the experiments, a pilot study was performed to identify any limitation in the range of motion of the upper extremity and shortness of the latissimus dorsi. Participants ranged from 21 to 24 years of age, mean height was 178.1 ± 5.6 cm, mean weight was 69.6 ± 8.5 kg, and the mean BMI was 21.8 ± 1.8 kg/m2. The ethics committee of the University of Inje approved this study, and all volunteers gave written informed consent before participation.
2.2. Electromyography A Trigno wireless system (Delsys, Boston, MA, USA) was used to obtain EMG signals. A single-channel surface electrode was placed at an oblique angle (25°) over the LD muscle on the dominant (right) side, approximately 4 cm below the inferior tip of the scapula and midway between the spine and lateral edge of the torso (Cram et al., 1998). The electrode was placed on the abdominal muscle site after inducing shoulder adduction, extension, and internal rotation in a seated position. Although one researcher placed the electrodes on all participants, the sites used differed among participants due to adduction, extension, and internal rotation. We placed the electrodes on abdominal muscle sites adjacent to those confirmed by geometric measurements. The skin site was initially prepared by shaving and abrasion, followed by cleaning with an alcohol swab to reduce impedance. The Trigno electrode used in this study has a band of 20–450 Hz and a commonmode rejection ratio of 80 dB. The researchers controlled data acquisition and processing on a laptop computer using EMGWorks software (Delsys Boston, MA, USA). Data were collected at a sampling rate of 2000 Hz and processed at 0.125-s intervals using the root mean square method. 2.3. Experimental procedures Resting EMG activity was recorded while the subject lay in a relaxed prone position. The participant was then asked to perform three trials of five isometric exertions believed to effectively activate the LD. Prior to testing, the participant was given 1 min of practice time for each exercise set. All exercises were performed for 5 s against manually applied resistance while the data were recorded, with a minimum 30-s rest between contractions. The participants rested for 5 min between exercise sessions. The order of exercise execution was randomized among participants. The five isometric exertions are described below (Fig. 1). (1) EP (Kendall et al., 2005; Hislop and Montgomery, 2002; Youdas et al., 2010): the participant lay prone on a bench with his arms by his sides and the shoulders internally rotated to create a palm-up position. From this position, the participant tried to move his shoulder toward the ceiling (extension). Downward manual resistance was applied to the forearm, and pressure was exerted on the contralateral side of the pelvis.
Fig. 1. The five exercises aimed at maximally activating the latissimus dorsi muscle. (1) Extension in Prone (EP), (2) caudal depression (CD), (3) body lifting (BL), (4) upper trunk bending (UTB), (5) Lat pull down (LPD).
Please cite this article in press as: Park S-y, Yoo W-g. Comparison of exercises inducing maximum voluntary isometric contraction for the latissimus dorsi using surface electromyography. J Electromyogr Kinesiol (2013), http://dx.doi.org/10.1016/j.jelekin.2013.05.003
3
S.-y. Park, W.-g. Yoo / Journal of Electromyography and Kinesiology xxx (2013) xxx–xxx
(2) Caudal depression (CD) (Hislop and Montgomery, 2002; Hughes and McBride, 2005): the participant lay prone on a bench with his arms by his sides and the shoulders internally rotated to create a palm-up position. He grasped handles located beside the bench and raised the right shoulder to chin level. The subject then tried to depress the right arm caudally while keeping the trunk (rib cage to pelvis) against the fixed handle. (3) BL (Hislop and Montgomery, 2002): the participant sat with his hands placed flat on tables located adjacent to the hips. Push-up handles and plates under the buttocks were used to ensure that the subject remained seated without flexing the elbow or depressing the shoulder. The subject then tried to depress his arms caudally and lift his body. Downward manual resistance was applied to the pelvis to prevent further elevation of the body. (4) Right and left UTB (Vera-Garcia et al., 2010): the participant attempted to bend the upper trunk laterally in the frontal plane while in the lateral decubitus position with the knees bent. The knees were secured with a belt, and the thorax and arms were braced manually by the researcher. (5) LPD (Snyder and Leech, 2009; Lehman et al., 2004; Signorile et al., 2002): in a seated position, the participant grasped a fixed crossbar using a wide grip with the elbows flexed to 90°. The participant was then asked to pull down on the bar as if attempting to break it. A researcher stabilized the participant by pressing downward on the shoulders to ensure that the contraction was isometric. The EMG values of the three trials were averaged. Of the five MVC techniques for the LD, the highest mean value was used to normalize the procedure (Vera-Garcia et al., 2010; Ekstrom et al., 2005 The intra-class correlation coefficient [ICC (3,1)] was P0.75 for each technique, which is regarded as good reliability (Fleiss, 1986). For statistical analyses, EMG data were expressed as a percentage of maximum EMG amplitude produced and referred to as the percentage of MVC (%MVC).
2.4. Statistical analysis The SPSS statistical package (version 18.0; SPSS, Inc., Chicago, IL, USA) was used to analyze differences in LD activation during the five normalization techniques. As a within-factor design, oneway repeated-measures analysis of variance was conducted to evaluate the differences in the% relative RMS–EMG among the five isometric MVC exercises. When necessary, post hoc Bonferroni corrections were performed to identify differences among the five exercises. All significance levels were set at P < 0.05. 3. Results Normalized EMG data for the LD differed significantly among normalization techniques. LD activation was increased significantly during EP compared with CD, BL, and UTB (P < 0.05; Fig. 2). The average%MVC was 92.62 ± 15.1 (95% confidence interval (CI) 85.57–100.69) in EP, 43.14 ± 19.23 (95% CI 32.88–53.39) in CD, 61.42 ± 27.38 (95% CI 46.83–76.02) in LB, 34.8 ± 15.36 (95% CI 26.62–42.99) in UTB, and 69.68 ± 30.49 (95% CI 53.43– 85.92) in LPD. The LPD resulted in significantly greater LD activation than did UTB (P 6 0.05; Fig. 2). Table 1 compares the%MVC values among the normalization techniques. 4. Discussion In the present study, we examined the EMG activity of the LD during five different normalization techniques. Research in kinesiology has demonstrated that this muscle contributes to shoulder extension, depression, adduction, and internal rotation, as well as trunk bending (Kendall et al., 2005; Hislop and Montgomery, 2002). The normalization techniques included in the present study induce at least some of these actions. Although previous clinical studies have used some or all of these techniques, differences among techniques have not been examined statistically. In the present study, LD activation was greatest during EP (8/16 partici-
Fig. 2. The normalized sEMG data (%MVC, mean ± SD) of the latissimus dorsi during the 5 different normalization techniques. ⁄Significant difference between techniques.
Table 1 Comparison of 5 different exercises using pair-wise comparison, mean differences and 95% confidence intervals (%MVC). Muscles
Exercises
Mean difference (95% CI) Extension prone
Latissimus dorsi
*
Caudal depression Lifting body Upper trunk bending Lat pull down
49.48* ( 31.19* ( 57.81* ( 22.94 (
67.03 31.93) 54.59 7.78) 73.57 42.05) 54.96 9.08)
Caudal depression
Lifting body
Upper trunk bending
– 18.28 ( 10.68 47.26) 8.33 ( 27.19 10.52) 26.54 ( 2.27 55.35)
– –
– – – 34.87* (4.91 64.83)
26.62 ( 46.08 7.15) 8.25 ( 21.01 37.52)
Significant difference between conditions.
Please cite this article in press as: Park S-y, Yoo W-g. Comparison of exercises inducing maximum voluntary isometric contraction for the latissimus dorsi using surface electromyography. J Electromyogr Kinesiol (2013), http://dx.doi.org/10.1016/j.jelekin.2013.05.003
4
S.-y. Park, W.-g. Yoo / Journal of Electromyography and Kinesiology xxx (2013) xxx–xxx
pants) or LPD (7/16 participants); in one participant, it was greatest during BL. Although no significant difference was observed between the EP and LPD techniques, the LPD data exhibited a lower average%MVC and greater variability (SD = 30.49) than the EP (SD = 15.1). When pulling the bar down with a flexed elbow and abducted shoulder, in addition to the LD and teres major, the posterior deltoid, biceps brachii, and pectoralis major could be recruited for shoulder adduction, elbow flexion, and scapular depression (Snyder and Leech, 2009, Sperandei et al., 2009). Large between-subject effects in the LPD may also have been present. Although we instructed the participants on how to perform the LPD and allowed them to practice, trained subjects might be able to alter their muscle activity voluntarily, emphasizing the LD (Snyder and Leech, 2009). The potential for recruiting a number of muscles during LPD exertion and differences among individuals might lead to large variability in the%MVC during LPD exertion. Our results demonstrated that LD activation was significantly greater during EP than during other exercises, except LPD. The mean difference between data obtained during EP and UTB and the calculation of MVC values >50% for EP and CD demonstrate that the inappropriate use of MVC can lead to the misinterpretation of exercise effects, such as the calculation of values representing >100% MVC or relatively higher%MVC values than obtained for other musculature. Three previous studies investigated the effects of pull-down exercises on LD activation (Koyama et al., 2010; Snyder and Leech, 2009; Signorile et al., 2002); two of these studies used the same EMG normalization method (LPD) and reported similar LD activation (70% MVC), whereas the third study (Koyama et al., 2010) used a similar exercise load but a different normalization technique (shoulder extension in the seated position, similar to EP) and reported an MVC of 50%. The only difference between the former two studies and the latter study was the normalization technique. We speculate that shoulder extension activates more LD muscle during the LPD than does shoulder adduction. The greater LD activation during MVC using shoulder extension reported in the third study compared with the first two studies is similar to our findings. Although we found no significant difference between EP and LPD, LD activation was greater in the EP than in the LPD, with a mean difference of 22% MVC. No participant showed maximal LD activation during CD or UTB. Although both of these exercises have been used to normalize EMG data for the LD (Vera-Garcia et al., 2010; Hughes and McBride, 2005), these results indicate that they induced less LD activation than did EP and LPD, with large mean differences. These differences between previous findings and our results may be due to differences in electrode placement on LD muscle sites rather than to errors in sEMG measurement. Previous studies of the trunk musculature during certain movements and postures described the sEMG site for the LD as ‘‘lateral to T9,’’ which is more medial and superior than the site used in the present study (Vera-Garcia et al., 2010; Drake et al., 2006). Paton and Brown (1995) suggested the possibility of functional differentiation within LD fibers, with caudal fibers of the LD preferentially activated in accordance with the direction of exertion at the shoulder t. This possibility means that movements such as UTB may activate other LD sites. Therefore, the%MVC results obtained in the present study may differ from those that would be obtained with the use of medial or superior LD sites. CD and BL, which are alternatives to EP, have been suggested to independently activate the LD muscle (Hislop and Montgomery, 2002). Both of these exercises aim to induce shoulder depression against resistance but result in less LD activation than do EP and LPD. Boettcher et al. (2008) recently demonstrated that normalization techniques for the LD involve internal rotation or extension of the shoulder t. Previous studies have not included shoulder
depression, preventing comparison with the present study, but our results suggest that CD might produce less accurate MVC values than do EP and LPD. Some limitations of this study should be considered. First, although the study compared normalization techniques for the LD muscle, it a small number of only male participants were included. Second, we used a single electrode site to measure the LD activity, whereas clinical studies generally use additional LD sites. Third, we could not record kinematic data throughout the experiment, preventing a numerical representation of the magnitudes of extension and internal rotation. Fourth, generalization to other populations, such as individuals with shoulder pathology, was not possible. Fifth, this study included only exercises that induce maximum voluntary isometric contraction, and any future study should include a submaximal task for the normalization procedure. 5. Conclusion This study compared normalization techniques for the LD with the aim of identifying an adequate method. We confirmed that EP, which is generally recommended in the clinical literature, resulted in more LD activation than did the other techniques. We also found that LPD is also effective for normalizing LD activation. Considering the muscle actions that occur during a pulling motion, the shoulder extension, adduction, and internal rotation components might be activated during performance of LD normalization techniques, causing error in the MVC calculation. Conflict of interest None declare Acknowledgement This research was ed by Basic Science Research Program through the National Research Foundation of Korea (NRF) funded by the Ministry of Education, Science and Technology (No. 2012R1A1B4001058). References Burden A. How should we normalize electromyograms obtained from healthy participants? What we have learned from over 25 years of research. J Electromyogr Kinesiol 2010;20(6):1023–35. Boettcher CE, Ginn KA, Cathers I. Standard maximum isometric voluntary contraction tests for normalizing shoulder muscle EMG. J Orthop Res 2008;26(12):1591–7. Cram JR, Kasman GS, Holtz J. Introduction to surface electromyography. 1st ed. Gaithersburg: Aspen; 1998. Drake JD, Fischer SL, Brown SH, Callaghan JP. Do exercise balls provide a training advantage for trunk extensor exercises? A biomechanical evaluation. J Manipulative Physiol Ther 2006;29(5):354–62. Ekstrom RA, Soderberg GL, Donatelli RA. Normalization procedures using maximum voluntary isometric contractions for the serratus anterior and trapezius muscles during surface EMG analysis. J Electromyogr Kinesiol 2005;15:418–28. Fleiss J. The design and analysis of clinical experiments. 1st ed. Canada: John Wiley and Sons; 1986. Hautier CA, Arsac LM, Deghdegh K, Souquet J, Belli A, Lacour JR. Influence of fatigue on EMG/force ratio and cocontraction in cycling. Med Sci Sports Exerc 2000;32(4):839–43. Hislop HJ, Montgomery J. Muscle testing and function. 7th ed. Philadelphia: WB Saunders; 2002. Hughes CJ, McBride A. The use of surface electromyography to determine muscle activation during isotonic and elastic resistance exercise for shoulder rehabilitation. Orthopaedic Practice 2005;17(2):18–23. Kendall FP, McCreary EK, Provance PG, Rodgers MM, Romani WA. Muscles: testing and function, with posture and pain. 5th ed. Baltimore, MD: Lippincott Williams & Wilkins; 2005. Koyama Y, Kobayashi H, Suzuki S, Enoka RM. Enhancing the weight training experience: a comparison of limb kinematics and EMG activity on three machines. Eur J Appl Physiol 2010;109(5):789–801.
Please cite this article in press as: Park S-y, Yoo W-g. Comparison of exercises inducing maximum voluntary isometric contraction for the latissimus dorsi using surface electromyography. J Electromyogr Kinesiol (2013), http://dx.doi.org/10.1016/j.jelekin.2013.05.003
S.-y. Park, W.-g. Yoo / Journal of Electromyography and Kinesiology xxx (2013) xxx–xxx Lehman GJ, Buchan DD, Lundy A, Myers N, Nalborczyk A. Variations in muscle activation levels during traditional latissimus dorsi weight training exercises: an experimental study. Dyn Med 2004;3(1):4. Paton ME, Brown JM. Functional differentiation within latissimus dorsi. Electromyogr Clin Neurophysiol 1995;35(5):301–9. Signorile JF, Zink AJ, Szwed SP. A comparative electromyographical investigation of muscle utilization patterns using various hand positions during the lat pulldown. J Strength Cond Res 2002;16(4):539–46. Smith J, Padgett DJ, Kaufman KR, Harrington SP, An KN, Irby SE. Rhomboid muscle electromyography activity during 3 different manual muscle tests. Arch Phys Med Rehabil 2004;85(6):987–92. Snyder BJ, Leech JR. Voluntary increase in latissimus dorsi muscle activity during the lat pull-down following expert instruction. J Strength Cond Res 2009;23(8):2204–9. Sperandei S, Barros MA, Silveira-Júnior PC, Oliveira CG. Electromyographic analysis of three different types of lat pull-down. J Strength Cond Res 2009;23(7):2033–8. Vera-Garcia FJ, Moreside JM, McGill SM. MVC techniques to normalize trunk muscle EMG in healthy women. J Electromyogr Kinesiol 2010;20(1):10–6. Youdas JW, Amundson CL, Cicero KS, Hahn JJ, Harezlak DT, Hollman JH. Surface electromyographic activation patterns and elbow t motion during a pull-up, chin-up, or perfect-pullup™ rotational exercise. J Strength Cond Res 2010;24(12):3404–14.
5
Won-gyu Yoo received the Ph.D. in Physical Therapy Treatments for Musculoskeletal Disorders from the Yonsei University, the Republic of Korea, in 2008. He was the acting head of the Department of Physical Therapy at Inje University in Gimhea, Gyeongsangnamdo, Republic of Korea. He is working as the main researcher of National Research Foundation of Korea for posture correction research of computer s. His research interests include biological signal processing, chronic muscle pain and dysfunction due to overuse, and medical device development for physical therapy interventions.
Se-yeon Park received his master of science in physical therapy at the Inje university in 2012 and now is a doctor of science student in physical therapy and rehabilitation sciences at Inje university. He is currently working as a researcher of National Research Foundation of Korea and a member of the Korean Physical Therapy Association. His research interests include musculoskeletal response in physical therapy interventions, and scapular dyskinesis.
Please cite this article in press as: Park S-y, Yoo W-g. Comparison of exercises inducing maximum voluntary isometric contraction for the latissimus dorsi using surface electromyography. J Electromyogr Kinesiol (2013), http://dx.doi.org/10.1016/j.jelekin.2013.05.003
Related Documents c2h70

Contraction For The Latissimus Dorsi Using Surface Electromyography 4n4l4b
December 2019 14
Muscle Contraction Project 1y4s33
December 2021 0
Jsa For Surface Coating 651e4w
May 2020 25
Parameter Settings For Electrically Stimulated Muscle Contraction 5c1m4t
October 2019 43
Abnormal Uterine Contraction 156w4c
November 2019 72
Contraction Surgery Lesson Plan 2o1e40
November 2019 24More Documents from "Rodrigo Albuquerque" 65g42

Encefalopatia Espongiforme Bovina 6i734
May 2020 21
Contraction For The Latissimus Dorsi Using Surface Electromyography 4n4l4b
December 2019 14
Cmc Rescue Mpd 's Manual 305d4s
November 2019 98
6g3p1u
March 2021 0
Planejamento Completo 2x3s2e
November 2019 37