Case Study Intestinal Obstruction 5h74x
This document was ed by and they confirmed that they have the permission to share it. If you are author or own the copyright of this book, please report to us by using this report form. Report 2z6p3t
Overview 5o1f4z
& View Case Study Intestinal Obstruction as PDF for free.
More details 6z3438
- Words: 10,588
- Pages: 68
Our Lady of Fatima University College of Nursing Valenzuela Campus
Intestinal Obstruction Partial Probably sec to Colonic Malignancy In Partial Fulfillment of requirements of NCM 107B RLE leading to the degree of Science in Nursing
A Case Study Presented to: Ms. Vanessa O. Umali, R.N. MAN
Presented by: Maria Paula M. Bungay July 26, 2015 TABLE OF CONTENTS
I. Introduction II. Objectives III. Patient’s Profile IV. Anatomy and Physiology V. Pathophysiology VI. Laboratory Examination Results VII. Gordon’s Assessment VIII. Nursing Care Plans IX. Drug Study X. Health Teachings
I. Introduction
2
In the present generation, we cannot deny the reality that different diseases sprout as life progresses. The world is in the generation where diseases are widespread and the medical fields are doing their further research in order to stop them. Being responsible for one’s health is very important for it builds the foundation of a healthy body. It is our choice to live a disease free body. It is always our choice of what food will you eat, how much sleep you need, etc. There are a lot of fashion trends in the world that will make each individual’s life a masterpiece, but the best fashion trend at present is a fit, healthy body. Intestinal obstruction is significant mechanical impairment or complete arrest of the age of contents through the intestine. Symptoms include cramping pain, vomiting, constipation, and lack of flatus. Diagnosis is clinical, confirmed by abdominal x-rays. Treatment is fluid resuscitation, nasogastric suction, and, in most cases of complete obstruction, surgery. According to Bordeianou and Yeh of Wolters Kluwers, Bowel obstruction occurs when the normal flow of intraluminal contents is interrupted. Obstruction can be functional (due to abnormal intestinal physiology) or due to a mechanical obstruction, which can be acute or chronic. Advanced small bowel obstruction leads to bowel dilation and retention of fluid within the lumen proximal to the obstruction, while distal to the obstruction, as luminal contents , the bowel decompresses. If bowel dilation is excessive, or strangulation occurs, perfusion to the intestine can be compromised leading to necrosis or perforation, complications, which increase the mortality, associated with small bowel obstruction. The most common causes of mechanical small bowel obstruction are postoperative adhesions and hernias. Other etiologies of small bowel obstruction include disease intrinsic to the wall of the small intestine (eg, tumors, stricture, intramural hematoma) and processes that cause intraluminal obstruction (eg, intussusception, gallstones, foreign bodies). Acute, mechanical small bowel obstruction is a common surgical emergency. It is estimated that over 300,000 laparotomies per year are performed in the United States for adhesion-related obstructions. Ischemia, which complicates 7 to 42 percent of bowel obstructions, significantly increases mortality associated with bowel obstruction. The small bowel is involved in about 80 percent of cases of mechanical intestinal obstruction. The incidence is similar for males and females. In one Polish study of adult
3
patients, the average age of patients with acute obstruction was 64 years, women comprised 60 percent of the group, and the small bowel was affected in 76 percent. In addition, I have learned and gained new knowledge regarding on Intestinal obstruction. The in-depth understanding of the etiology, pathophysiology, clinical manifestations, diagnosis, treatment and prevention of this condition has yield and enhanced my acquired knowledge. As a student nurse, I also believed that actual interaction with the patient who has the condition being studied can make it easier to understand. Also, to be able to learn completely, one must be able to know how the concepts learned be applied into the actual clinical practice. The knowledge I acquired through this study will give me the opportunity to improve my capability to deliver efficient and appropriate interventions and information to a variety of population. The knowledge, skills and attitude that comprise an effective nurse will be of high regard to promote a reduction in the morbidity and mortality rate. (http://www.uptodate.com/).
II. Objectives Nurse-Centered
4
After the completion of this case study, the nurse will be able to: 1.
Understand the current statistics and latest trend regarding Intestinal Obstruction partial probably sec to Colonic Malignancy.
2.
Describe factually, the personal and pertinent family history of the patient and relate it to the present condition.
3.
Perform comprehensive physical assessment.
4.
Trace the book-based and client-centered pathophysiology of Intestinal Obstruction partial probably sec to Colonic Malignancy.
5.
Determine the predisposing and precipitating factors and the signs and symptoms and relate to the disease process.
6.
Enumerate and describe the diagnostic and laboratory procedures as well as the nursing responsibilities in relation to the disease condition
7.
Enumerate the different treatment modalities and their indication specifically for the patient’s condition.
8.
Identify the pharmacologic treatment provided to the patient, relate the actions of each drug with the disease process and evaluate the patient’s response to the medications given.
9.
Identify nursing diagnoses, formulate short-term goals, carry out appropriate interventions and evaluate the plan.
10. Appraise the effectiveness of medical and surgical nursing management in treating the patient. 11. List the preventive measure for the occurrence of Intestinal Obstruction partial probably sec to Colonic Malignancy for the benefit of the general public. Patient –Centered After the completion of this case study, the patient will be able to: 1. Report understanding of the disease process. 2. Understand the indications of the different diagnostic procedures and medical management involved in her care. 3. Cooperate with the necessary medical and nursing interventions. 4. Adhere with the health teachings provided. 5. Understand the different ways of health promotion and prevention in relation to the disease condition.
5
6. Demonstrate improved conditions as evidenced by absence of further complications. III. Patient’s Profile Name: Mr. Isaw Age: 62 years old Birthday: February 18, 1952 Nationality: Filipino Religion: Roman Catholic Civil Status: Married Date ission: July 2, 2015 Time of ission: 12:15 PM Chief Complaint's: Abdominal Pain Initial Diagnosis: Intestinal Obstruction Partial Probably sec to Colonic Malignancy Final Diagnosis: None
HISTORY OF PAST ILLNESS During the previous years, Mr. Isaw was diagnosed Hypertensive in 2014 and a history of vehicular accident 20 years ago, which affected his Left femur. He is a non-smoker and non-alcoholic. As for childhood illness, he had chicken pox and measles. He also experienced coughs and colds for common illness. To relieve symptoms, he would take different herbal plants or purchase over-the-counter drugs. For the herbal plants, he prepares decoction with one to two glasses of water for fifteen minutes or until one half of the liquid is left. Then, he will drink it. He also experienced fever once in a while in which he takes over-the-counter drugs. Mr. Isaw, has no family history of hypertension, Diabetes, Arthymias, Pulpomonary Tuberculosis, and Cancer. For food allergies, crab and shrimp are contraindicated but no allergies to drugs. HISTORY OF PRESENT ILLNESS Prior to ission, Mr. Isaw complained of sudden onset abdominal pain described as bloatedness more prominent in the epigastric and right periumbilical area. There was no
6
associated nausea, vomiting, change in bowel habits, hematochezia, melena, jaundice and fever. Patient consulted at PGH, Abdominal X-ray revealed dilated small bowels. He was then referred to the institution for further management. PHYSICAL ASSESSMENT Physician’s Physical Assessment done by the Resident on Duty (July 2, 2015, lifted from the patient's chart) Height: 5’6 Weight: 81 kg Vital Signs as follows: T: 36.9 °C
PR: 116 bpm
RR: 18m
BP: 150/90 mmHg
SAO2: 97%
GENERAL SURVEY Mr. Isaw, Assessed/received patient lying on bed, awake, conscious, responsive, and coherent. With the following vital signs: Temperature: 36.7 °C Heart rate: 70 bpm Respiratory rate: 20 bpm Blood Pressure: 140/90 mmHg SAO2: 96% NUTRITIONAL STATUS Upon ission, Mr. Isaw was placed on NPO and IVF of D5LR 1 x Q8. CBC, BT, PTPTT, FBS, BUN, CREA, Na, K, Cl, 12-LECG, Chest X-ray PA, abdominal series, and Urinalysis were requested. NGT and Foley Catheter were inserted.
SKIN
7
> Pallor noted. > Good skin turgor in both upper and lower extremities; the skin returns to its previous state immediately after being tented. > warm moist skin, no active dermatoses. HAIR > Hair is black and is evenly distributed. > Silky and smooth hair. > No areas of hair loss noted. > Thick hair strands. NAILS > Trimmed clean nails. > Concave shaped; with a nail plate angle of about 160 degrees. > Smooth in texture. > Intact epidermal lining around the nails. > Capillary Refill Test less than 3 seconds. SKULL AND FACE > Rounded (normocephalic and symmetrical with frontal, parietal and occipital prominences). > Head has no cervical lymphadenophaties > No nodules or masses upon palpation. EYES AND VISION
8
> Eyebrows and eyelashes are evenly distributed. > Eyelids are intact > Pink palpebral conjuctiva > Sclera appears white. > Pale conjunctiva. > No discharges and discoloration noted. > Blink reflex intact. EARS AND HEARING > Ears are symmetrical in size and in line with the outer canthus of the eyes. > Color of ears is the same with the facial skin. > No discharges and foul odor noted upon inspection. > Pinna and ear canal are clean. > Auricles are firm and recoil to previous state when folded. > No nodules or masses noted upon palpation NOSE AND SINUSES > No nasal discharge > No tenderness masses and pain noted upon palpation OROPHARYNX (Mouth and Throat) > Dry and pale lips noted upon inspection > Tongue is able to move freely
9
> Good oral hygiene. > Thyroid gland moves with deglutition NECK > Jugular vein is not visible > Muscles are equal in size with the head centered > Slow muscle movement > Lymph nodes are not palpable CARDIOVASCULAR AND PERIPHERAL SYSTEM > Skin color of palm of the hand and feet is pink. > Pink nail beds upon inspection. > Symmetric pulse volumes, full pulsations of peripheral pulses. > Heart rate is 70 beats per minute. > Blood Pressure is 140/90 mmHg > (Vital signs taken during the time of assessment July 2, 2015 at 0715H) RESPIRATORY SYSTEM > + DOB > Symmetric chest expansion > Skin and chest wall are intact and has uniform temperature > No tenderness and masses noted upon palpation > Regular breathing pattern
10
> Presence wheezing and crackles sound upon auscultation > Full and symmetric chest wall expansion BREAST AND AXILLAE > Breasts are symmetrical in size; color is the same as with the abdomen. > Both nipples are symmetrical in size. > No discharges noted. > No tenderness, masses, and nodules noted upon palpation. ABDOMEN > Direct tenderness at epigastric area. > Abdominal skin is intact. > Distended abdomen noted. > Audible bowel sound upon auscultation. > Abdominal dullness upon percussion. MUSCULOSKELETAL > Posture is good, able to stand straight and can walk alone properly but slowly > Scar at left thigh and right medial leg and foot NEUROLOGIC >with a GCS of 15 > Patient has times of looking in the distance and is slow in response when a question asked.
11
> Patient was able to answer well when asked of her complete name, birth date and age. URINARY SYSTEM > Patient has indwelling Foley Catheter REPRODUCTIVE SYSTEM > The patient refused to be assessed with her external reproductive organ but she verbalized that she has minimal vaginal bleeding and complain of pain when secretions are expelled. REVIEW OF SYSTEM Integumentary System The patient has no history of bruises in both upper and lower extremities. Head The patient had no history of any form of head injuries. Eyes Patient had no history of any eye problems. Ears and Hearing Patient had no history of smelly discharges on both ears, and no complaints of hearing impairment. Breast and Axillae The patient had no history of breast nodules, no enlargement, no tenderness, no pain and unusual discharges. Respiratory System
12
The patient has no history of asthma or other respiratory problems. Cardiovascular System The patient has a history of hypertension. Genitourinary System The patient had no history of any genital problems. Usually urinates 5 times a day. Gastrointestinal System The patient had experienced abdominal pain. Musculoskeletal System Patient has no history of t pain. Neurologic System Patient had no history of any major mental problems.
Cranial Nerve Assessment:
13
CRANIAL NERVE
ASSESSMENT TECHNIQUE
EXPECTED OUTCOME
ACTUAL FINDINGS
I: Olfactory Type: Sensory Function: Smell
Ask the client to identify a scented object that you are holding.
Client is able to identify different smell with each nostril separately and with eyes closed unless such condition like colds is present.
The client was able to identify the aromas of cologne and alcohol that she had smelled.
II: Optic Type: Sensory Function: Vision
Provide adequate lighting and ask client to read words on a newspaper held at a distance of 36 cm (14 inches) with each eye first then both eyes.
The client should be able to read with each eye and both eyes.
The client was able to read the words in the newspaper at 14 inches.
III: Oculomotor, IV: Trochlear & VI: Abducens Type: Motor Function: Upward and Downward movement of Pupils.
-Hold a penlight 1 ft. -Client’s eyes should in front of the client’s be able to follow the eyes. Ask the client to penlight as it moves. follow the movements of the penlight with the eyes only. Move the penlight upward, downward, sideward and diagonally. -Ask the client to look straight ahead then approach the pupil with a penlight and observe for pupil constriction.
-The client’s eyes will have a normal reaction for PERRLA.
-Both eyes of the client were able to follow the Penlight’s movements.
-The client had a normal reaction to PERRLA as Pupils are equally round, reactive to light and accommodation.
V: Trigeminal Type: Sensory Function: Sensation of cornea
While client looks upward, lightly touch the lateral sclera of eye to elicit blink reflex.
Client should have a positive corneal reflex.
The client was able to elicit corneal reflex.
VII: Facial Type: Motor Function: Facial movements
Ask client to: smile, frown and wrinkle forehead, show teeth, puff out cheeks,
Client should smile, frown and wrinkle forehead, show teeth, puff out cheeks,
The client was able to do the facial movements symmetrically.
14
purse lips, raise eyebrows, close eyes tightly against resistance
purse lips, raise eyebrows, close eyes tightly against resistance. Movements are symmetrical.
VIII: Vestibulocochlear/ acoustics Type: Sensory Function: Hearing
Have the Client occlude one ear. Out of the client’s sight, place a tickling watch 2 cm. Ask what the client can hear and repeat with the other ear.
Client should be able to hear the ticking of the watch in both ears.
The client was able to hear the ticking of the watch in both ears.
IX. Glossopharyngeal & X: Vagus Type: Motor Function: Swallowing and Speaking
Ask the client to swallow and say its name.
The client should be able to swallow without difficulty and speak audibly.
The client was able to swallow without difficulty and speak audibly.
XI. Spinal Accessory Type: Motor Function: strength and resistance
-Ask client to shrug the shoulders against your hands.
-There is symmetric, strong contraction of the trapezious muscles.
The client was able to symmetrically contract the trapezious muscle.
-Ask client to turn the head against resistance, first to the right then to the left, to assess the sternocleidomastoid muscle.
-There is strong contraction of the sternocleidomastoid muscle on the side opposite to the turned face.
-The client was able to contract strenocleidomastoid muscleon the side opposite to the turned face.
Ask the client to protrude the tongue and move in different directions.
The client will be able to protrude her tongue and move in different directions.
The client was able to protrude his tongue and move it in different directions.
XII: Hypoglossal Type: Motor Function: Movement and strength of tongue
15
IV. Anatomy and Physiology The digestive system, sometimes called the gastrointestinal tract, alimentary tract, or gut, consists of a long hollow tube which extends through the trunk of the body, and its accessory structures: the salivary glands, liver, gallbladder, and pancreas. The digestive tract is divided into two sections, the upper tract, consisting of the mouth, esophagus, and stomach, and the lower tract, consisting of the intestines. FIGURE 20-1 Anatomy of the digestive system with associated events.
Inside this tube, ingested food and fluid, along with secretions from various glands, are efficiently processed. First, they are broken down into their separate constituents; then the desired nutrients, water, and electrolytes are absorbed into the blood for use by the cells, and waste elements are eliminated from the body. Within this system, the liver can reassemble the
component nutrients into new materials as they are needed by the body. For example, the proteins in milk are digested by enzymes in the digestive tract, producing the component amino acids, which are then absorbed into the blood. The individual amino acids are used by the liver cells to produce new proteins, such as albumin or prothrombin, or they may circulate as they are in the amino acid pool in the blood to be taken up by individual cells as necessary. The peritoneal cavity refers to the potential space between the parietal and visceral peritoneum. A small amount of serous fluid is present in the cavity to facilitate the necessary movement of structures such as the stomach. Numerous lymphatic channels drain excessive fluid from the cavity. Because serous membranes are normally thin, somewhat permeable, and highly vascular, the peritoneal membranes are useful as an exchange site for blood during peritoneal dialysis in patients with kidney failure. However, such an extensive membrane may also facilitate the spread of infection or malignant tumor cells throughout the abdominal cavity or into the general circulation. The mesentery is a double layer of peritoneum that s the intestines and conveys blood vessels and nerves to supply the wall of the intestine. The mesentery attaches the jejunum and ileum to the posterior (dorsal) abdominal wall. This arrangement provides a balance between the need for of the intestines and the need for considerable flexibility to accommodate peristalsis and varying amounts of content. The greater omentum is a layer of fatty peritoneum that hangs from the stomach like an apron over the anterior surface of the transverse colon and the small intestine. The lesser omen-tum is part of the peritoneum that suspends the stomach and duodenum from the liver. When inflammation develops in the intestinal wall, the greater omentum, with its many lymph nodes, tends to adhere to the site, walling off the inflammation and temporarily localizing the source of the problem. Inflammation of the omentum and peritoneum may lead to scar tissue and the formation of adhesions between structures in the abdominal cavity, such as loops of intestine, restricting motility and perhaps leading to obstruction. Intestinal Obstruction Intestinal obstruction refers to a lack of movement of the intestinal contents through the intestine. Because of its smaller lumen, obstructions are more common and occur more rapidly in the small intestine, but they can occur in the large intestine as well. Depending on the cause and location, obstruction may manifest as an acute problem or a gradually developing situation. For example, twisting of the intestine could cause sudden total obstruction, whereas
a tumor leads to progressive obstruction. FIGURE 20-37 Colostomy. A, sigmoid colostomy-a surgically created opening into the colon through the abdominal wall. B, The stoma is the new opening on the abdomen. It is always red and moist, is not painful, but may bleed easily. C, A plastic pouch to collect stools is attached to the stoma. (Courtesy of Hollister Incorporated, Patient Education Series.)
Intestinal obstruction occurs in two forms. Mechanical obstructions are those resulting from tumor, adhesions, hernias, or other tangible obstructions. Functional, or adynamic, obstructions result from neurologic impairment, such as spinal cord injury or lack of propulsion in the intestine, and are often referred to as paralytic ileus. While the end result can be the same, these types manifest somewhat differently and require different treatment.
Colon The colon is the last part of the digestive system in most vertebrates; it extracts water and salt from solid wastes before they are eliminated from the body, and is the site in which flora-aided (largely bacteria) fermentation of unabsorbed material occurs. Unlike the small intestine, the colon does not play a major role in absorption of foods and nutrients. However, the colon does absorb water, potassium and some fat soluble vitamins. In mammals, the colon consists of four sections: the ascending colon, the transverse colon, the descending colon, and the sigmoid colon (the proximal colon usually refers to the ascending colon and transverse colon). The colon, cecum, and rectum make up the large intestine. The location of the parts of the colon are either in the abdominal cavity or behind it
in
the retroperitoneum. The colon in those areas is fixed in location. Arterial supply to the colon comes from branches of the superior mesenteric artery (SMA) and inferior mesenteric artery (IMA). Flow between these two systems communicates via a "marginal artery" that runs parallel to the colon for its entire length. Historically, it has been believed that the arc of Riolan, or the meandering mesenteric artery (of Moskowitz), is a variable vessel connecting the proximal SMA to the proximal IMA that can be extremely
important if either vessel is occluded. However, recent studies conducted with improved imaging technology have questioned the actual existence of this vessel, with some experts calling for the abolition of the from future medical literature. Venous drainage usually mirrors colonic arterial supply, with the inferior mesenteric vein draining into the splenic vein, and the superior mesenteric vein ing the splenic vein to form the hepatic portal vein that then enters the liver. Lymphatic drainage from the entire colon and proximal two-thirds of the rectum is to the paraaortic lymph nodes that then drain into the cisterna chyli. The lymph from the remaining rectum and anus can either follow the same route, or drain to the internal iliac and superficial inguinal nodes. The pectinate line only roughly marks this transition. Ascending colon The ascending colon, on the right side of the abdomen, is about 25 cm long in humans. It is the part of the colon from the cecum to the hepatic flexure (the turn of the colon by the liver). It is secondarily retroperitoneal in most humans. In ruminant grazing animals, the cecum empties into the spiral colon. Anteriorly it is related to the coils of small intestine, the right edge of the greater omentum, and the anterior abdominal wall. Posteriorly, it is related to the iliacus, the iliolumbar ligament, the quadratus lumborum, the transverse abdominis, the diaphragm at the tip of the last rib; the lateral cutaneous, ilioinguinal, and iliohypogastric nerves; the iliac branches of the iliolumbar vessels, the fourth lumbar artery, and the right kidney. The ascending colon is supplied by parasympathetic fibers of the vagus nerve (CN X). Arterial supply of the ascending colon comes from the ileocolic artery and right colic artery, both branches of the SMA. While the ileocolic artery is almost always present, the right colic may be absent in 5–15% of individuals. Transverse colon The transverse colon is the part of the colon from the hepatic flexure to the splenic flexure (the turn of the colon by the spleen). The transverse colon hangs off the stomach, attached to it by a wide band of tissue called the greater omentum. On the posterior side, the transverse colon is connected to the posterior abdominal wall by a mesentery known as the transverse mesocolon. The transverse colon is encased in peritoneum, and is therefore mobile (unlike the parts of the colon immediately before and after it). Cancers form more frequently further along the large intestine as the contents become more solid (water is removed) in order to form feces. The proximal two-thirds of the transverse colon is perfused by the middle colic artery, a branch of SMA, while the latter third is supplied by branches of the IMA. The "watershed" area
between these two blood supplies, which represents the embryologic division between the midgut and hindgut, is an area sensitive to ischemia. Descending colon The descending colon is the part of the colon from the splenic flexure to the beginning of the sigmoid colon. The function of the descending colon in the digestive system is to store food that will be emptied into the rectum. It is retroperitoneal in two-thirds of humans. In the other third, it has a (usually short) mesentery. The arterial supply comes via the left colic artery. Sigmoid colon The sigmoid colon is the part of the large intestine after the descending colon and before the rectum. The name sigmoid means S-shaped (see sigmoid). The walls of the sigmoid colon are muscular, and contract to increase the pressure inside the colon, causing the stool to move into the rectum. The sigmoid colon is supplied with blood from several branches (usually between 2 and 6) of the sigmoid arteries, a branch of the IMA. The IMA terminates as the superior rectal artery. Sigmoidoscopy is a common diagnostic technique used to examine the sigmoid colon. Redundant colon One variation on the normal anatomy of the colon occurs when extra loops form, resulting in a longer than normal organ. This condition, referred to as redundant colon, typically has no direct major health consequences, though rarely volvulus occurs resulting in obstruction and requiring immediate medical attention.[4] A significant indirect health consequence is that use of a standard adult colonoscope is difficult and in some cases impossible when a redundant colon is present, though specialized variants on the instrument (including the pediatric variant) are useful in overcoming this problem. Standing gradient osmosis Water absorption at the colon typically proceeds against a transmucosal osmotic pressure gradient. The standing gradient osmosis is a term used to describe the reabsorption of water against the osmotic gradient in the intestines. This hypertonic fluid creates an osmotic pressure that drives water into the lateral intercellular spaces by osmosis via tight junctions and adjacent cells, which then in turn moves across the basement membrane and into the capillaries. Functions of the Colon
There are differences in the large intestine between different organisms, the large intestine is mainly responsible for storing waste, reclaiming water, maintaining the water balance, absorbing some vitamins, such as vitamin K, and providing a location for flora-aided fermentation.Vitamin K is essential as a coagulation factor. By the time the chyme has reached this tube, most nutrients and 90% of the water have been absorbed by the body. At this point some electrolytes like sodium, magnesium, and chloride are left as well as indigestible parts of ingested food (e.g., a large part of ingested amylose, protein which has been shielded from digestion heretofore, and dietary fiber, which is largely indigestible carbohydrate in either soluble or insoluble form). As the chyme moves through the large intestine, most of the remaining water is removed, while the chyme is mixed with mucus and bacteria (known as gut flora), and becomes feces. The ascending colon receives fecal material as a liquid. The muscles of the colon then move the watery waste material forward and slowly absorb all the excess water. The stools get to become semi solid as they move along into the descending colon. The bacteria break down some of the fiber for their own nourishment and create acetate, propionate, and butyrate as waste products, which in turn are used by the cell lining of the colon for nourishment. No protein is made available. In humans, perhaps 10% of the undigested carbohydrate thus becomes available; in other animals, including other apes and primates, who have proportionally larger colons, more is made available, thus permitting a higher portion of plant material in the diet. This is an example of a symbiotic relationship and provides about one hundred calories a day to the body. The large intestine produces no digestive enzymes -— chemical digestion is completed in the small intestine before the chyme reaches the large intestine. The pH in the colon varies between 5.5 and 7 (slightly acidic to neutral).
Colonic Carcinoma / Colon Carcinoma / Colon Cancer Definition: It is a disease in which malignant (cancer) cells form in the tissues of the colon. The colon is part of the body's digestive system. The digestive system removes and processes nutrients (vitamins, minerals, carbohydrates, fats, proteins, and water) from foods and helps waste material out of the body. The digestive system is made up of the esophagus, stomach, and the small and large intestines. The first 6 feet of the large intestine are called the large bowel or colon. The last 6 inches are the rectum and the anal canal. The anal canal ends at the anus (the opening of the large intestine to the outside of the body). Risk Factors: Age and health history can affect the risk of developing colon carcinoma . Risk factors include the following:
Age 50 or older.
A family history of carcinoma of the colon or rectum.
A personal history of carcinoma of the colon, rectum, ovary, endometrium, or breast.
A history of polyps in the colon.
Signs and Symptoms:
A change in bowel habits.
Blood (either bright red or very dark) in the stool.
Diarrhea, constipation, or feeling that the bowel does not empty completely.
Stools that is narrower than usual.
Frequent gas pains, bloating, fullness, or cramps.
Weight loss for no known reason.
Feeling very tired.
Vomiting. A specimen removed from a patient with colonic carcinoma
V. Pathophysiology Pathophysiology of Intestinal obstruction
Risk Factors for Intestinal obstruction
Crohn’s disease – narrows intestinal ageways due to thickening Abdominal Cancer
2 types of obstructions
Mechanical: (+) Physical obstruction or increased pressure from walls creating a blockage
(+) Increased fluid and gas
Functional: Intestinal muscles cannot propel the contents along the bowel
Increased pressure on intestinal wall causes more fluid to enter intestine
(+) Severe vomiting & pain
(+) Dehydration & Electrolyte Imbalance
Decreased blood pressure &pressure on Continued hypovolemic shock intestinal wall causes edema, ischemia and decreased peristalsis
(+) Increased peristalsis attempts to force contents past obstruction
(+) Abdominal distention
Prolonged ischemia causes increased permeability and necrosis of wall. Intestinal bacteria & toxins leak into blood.
(+) mass in the small intestine
Pathophysiology of Colon Cancer
Predisposing factors: (+) Age (56% >70yrs old) Colorectal polyps Family history Previous colorectal cancer Ulcerative colitis /colonic crohn’s disease
Diagnostic test: Fecal occult blood test SigmoIdoscopy Digital Rectum Exam
Surgical Treatment: Colonoscopy Virtual Colonoscopy
Precipitating factors: Patient broke her right leg due to falling on the stairs Precipitating factors: Diet – high fat/low fiber Smoking Alcohol drinking (+)Lack of exercise
Etiology: Unknown
Abnormal proliferation of cells in the colon area
Signs and Symptoms: Rectal bleeding Bloody stools (+) Abdominal pain (+) Fatigue Constipation (+)Diarrhea
Arising from epithelial lining of the intestine
Benign polyps occur
(+) Nausea and Vomiting
Continuous plorifetation of cells in the polyps
Polypectomy Reduction likelihood of regrowth
Increase in size of the polyps
Exposure to carcinogens
Development of malignant tumor
Uncontrolled Increase in proliferation COLON CANCER size of cells in the tumor
Complications DEATH occur
Diagnostic test: SigmoIdos copy
VI.
Laboratory Examination
Results Diagnostic/ Laboratory Procedures
Date ordered Date results in
1. Complete Blood Count
Indications or Purposes
Results
Normal Value (Units used in the hospital)
Analysis and Interpretation of results
Hgb: 153
N: 115-175 g/L
The hemoglobin level is normal. This indicates that RBC is capable of carrying O2 and CO2 throughout the body.
Hct: 0.44
N: 0.40-0.52
The result indicates there is normal concentration of RBC within the blood
CBC is a screening test, used to diagnose and manage numerous diseases. The results can reflect problems with fluid or loss of blood.
a. Hemoglobin
Date ordered/ Date of Results: July 2, 2015
b. Hematocrit
Date ordered/ Date of Results: July 2, 2015
Hemoglobin determines the RBC that carries oxygen and carbon dioxide throughout the body
Hematocrit determines the
concentration of RBC within the blood volume c. RBC Date ordered/ Date of Results: July 2, 2015
volume.
RBC: 4.93
N:4.5-6.2
The result is within normal range which indicates that the body's RBCs containing hemoglobin, carrying oxygen to the body's tissues are functioning normally.
WBC: 13.0
N: 5-10x 109/L
WBC is high which indicates that there is infection presented in the body.
An RBC count is a blood test that measures how many red blood cells (RBCs) you have. RBCs contain hemoglobin, which carries oxygen. How much oxygen your body tissues get depends on how many RBCs you have and how well they work.
d. WBC Date ordered/ Date of Results: July 2, 2015
White blood cells (WBCs), also called leukocytes, are an important part of the immune system. These cells help
fight infections by attacking bacteria, viruses, and germs that invade the body. White blood cells originate in the bone marrow, but circulate throughout the bloodstream.
DIFFERENTIAL COUNT
a. Segmenters Segmenters: 0.84 Date ordered/ Date of Results: July 2, 2015
A type of white blood cell that respond to bacterial infections. Where the blood count has high levels of segmenters, this indicates the presence of a bacterial infection. Where there is a low level of segmenters, the patient is likely to be suffering from a viral infection or
N: 0.55-0.65
The result is higher than the normal range. Which indicates presence of bacterial infection.
an autoimmune disease.
b.Lymphocytes
Lymphocytes: 0.27 Date ordered/ Date of Results: July 2, 2015
Lymphocytes are responsible for immune responses. There are two main types of lymphocytes: B cells and T cells. The B cells make antibodies that attack bacteria and toxins while the T cells attack body cells themselves when they have been taken over by viruses or have become cancerous. Lymphocytes secrete products (lymphokines) that modulate the functional activities of many other types of cells and are often present at sites of chronic inflammation.
N: 0.25-0.35
Normal count of lymphocytes indicates that there is no presence of infection in the body
c. Eosinophils
N: 0.02-0.04 0.00 Date ordered/ Date of Results: July 2, 2015
Eosinophils are a specific type of white blood cell that protects your body against certain kinds of germs, mainly bacteria and parasites. They're also what causes you to have allergic reactions.
d. Monocytes Date ordered/ Date of Results: July 2, 2015
The result is below the normal range. Which indicates no significant.
0.06 Monocytes are a type of white blood cell that fights off bacteria, viruses and fungi. Monocytes are the biggest type of white blood cell in the immune system. Originally formed in the bone marrow, they are released into our blood and tissues. When certain germs enter the body, they quickly rush
N: 0.03-0.06
The result is normal. Which indicates that the body can fights off bacteria, virus and fungi,
to the attack.
site
for
e. Basophils Date ordered/ Date of Results: July 2, 2015
N: 0.00-0.01
Platelet Count: 311
Platelet Count: 150- 400 x 109/L
Basophils are granulocytic white blood cells that are active in the inflammatory response. They are mostly found in the skin and mucosa tissues, which are the tissues lining the openings into the body. They represent about 1% of all white blood cells in the body.
Platelet Count Date ordered/ Date of Results: July 2, 2015
0.00
A platelet count is a test to measure how many platelets you have in your blood. Platelets are parts of the blood that help the blood clot. They are smaller than red
The result is normal, which indicates that body is active for inflammatory response.
The result is within the normal range indicates that there is enough platelet produces for coagulation.
or white cells.
blood
Nursing Responsibilities: BEFORE 1. Explain to the patient the procedure and its purposes. 2. If the patient has eaten a meal with high sodium content in the past 24 hours, this should be noted. 3. Be sure not to draw blood, which has infused IVF. 4. Note if patient’s on a diet that restricts sodium and other nutrients. 5. Note other conditions such as diabetes. 6. Carefully watch for signs of electrolyte imbalance. 7. Perform a complete cephalocaudal assessment especially cardiac assessment and vital signs. 8. Make sure to have the right patient, specimen and method. DURING 1. Clean injection site with alcohol. 2. Lower the patient’s arm to dilate the veins. 3. Apply tourniquet and ask the patient to open and close fist. 4. Remove the tourniquet when drawing the final tube of blood. AFTER 1. Note for any signs of discomfort or bruising at the puncture site. 2. Provide pressure at the puncture site to stop bleeding and reduce bruising. 3. Apply warm compress to puncture site to relieve discomfort. 4. Send the specimen at the laboratory.
B. Blood Chemistry Diagnostic/ Laboratory Procedures
Date ordered Date results in
Indications or Purposes
Date ordered:
A serum creatinine test — which measures the level of creatinine in your blood — can indicate whether your kidneys are working properly.
70.10 umol/L
It regulates body water along with potassium. It is responsible for nerve conduction and contraction of muscle.
Na: 141
Results
Normal Value (Units used in the hospital)
Analysis and Interpretation of results
2. CLINICAL CHEMISTRY TEST
Creatinine
July 2, 2015 Date of Results: July 2, 2015
Sodium
Date ordered: July 2, 2015 Date of Results: July 2, 2015
N: 71-115 umol/L
The result is lower than the normal range which indicate that the kidney has a slightlyl glomerular filtration and renal damage. Creatinine is more accurate for renal condition.
N: 135-148 mmol/L
The result is within normal range, it indicates no presence of hypernatremia or hyponatremia
Potassium
Date ordered: July 2, 2015 Date of Results: July 2, 2015
Chloride
Date ordered: July 2, 2015 Date of Results: July 2, 2015
It is a mineral, which with Sodium and Calcium maintains normal heart rhythm and regulates water balance. A chloride test measures the level of chloride in your blood or urine. Chloride is one of the most important electrolytes in the blood. It helps keep the amount of fluid inside and outside of your cells in balance. It also helps maintain proper blood volume, blood pressure, and pH of your body fluids. Tests for sodium, potassium, and bicarbonate are usually done at the same time as a blood test for chloride.
K: 4.10
104.4
N: 3.5-5.3 mmol/L
N: 98-107 mmol/L
The result is within normal range, which indicates no presence of hyperkalemia or hypokalemia
The result is within normal range, which indicates there is normal functioning of the muscles, heart, and nerves. Which is also essential for normal fluid absorption and excretion.
Alanine Aminotrans liquid
Date ordered: July 2, 2015 Date of Results: July 2, 2015
Aspartate Aminotrans liquid
Date ordered: July 2, 2015 Date of Results: July 2, 2015
The blood test for aspartate aminotransferase (AST) and alanine aminotransferase (ALT) are usually used to detect liver damage. It is often ordered to screen for and/or help diagnose liver disorders. In the patient’s case, liver function is monitored due to metastasis of his cancer to his liver. The blood test for aspartate aminotransferase (AST) and alanine aminotransferase (ALT) are usually used to detect liver damage. It is often ordered to screen for and/or help diagnose liver disorders. In the patient’s case, liver function is monitored due to metastasis of his cancer to his liver.
19.0 U/L
18.6 U/L
N:10.0-44.0
N: 10.0-34.0
The result is within the normal range. Which indicates that liver is functioning normally.
The result is within the normal range. Which indicates that liver is functioning normally.
Calcium Gen 2
Date ordered: July 2, 2015 Date of Results: July 2, 2015
The Calcium Gen.2 assay is an in vitro diagnostics reagent system intended for the quantitative determination of calcium in human serum, plasma, and urine on Roche/Hitachi cobas c systems. Calcium measurements are used in the diagnosis and treatment of parathyroid disease, a variety of bone diseases, chronic renal disease, and tetany.
2.18 mmol/L
N: 2.20-2.75
The result is within the normal range.
NURSING RESPONSIBILITIES BEFORE 1. Confirm the patient’s identity using two patient identifiers according to facility policy. 2. Explain the procedure and the indication. 3. Inform the patient that the test requires blood sample, and explain that he may experience slight discomfort from the tourniquet and the needle puncture. 4. Instruct the patient that he doesn’t need to restrict food and fluids. For triglycerides she should not eat 12 hours before procedure. 5. Notify the laboratory and practitioner about any medications the patient is taking that may affect test results; they may need to be restricted. DURING 1. Perform venipuncture and collect the sample in a 3- or 4-mL clot activator tube. 2. Handle sample gently to prevent hemolysis. AFTER 1. A report of the results will be sent to the requesting Health Care Provider, who will discuss the results with the patient. 2. Depending on the results of this procedure, additional testing may be performed to evaluate or monitor progression of the disease process and determine the need for a change in therapy. 3. Evaluate test results in relation to the patient's symptoms and other tests performed.
Diagnostic/ Laboratory Procedures
Date ordered Date results in
2. Urinalysis
Date ordered: July 2, 2015 Date of Results: July 2, 2015
Indications or Purposes
Urinalysis yields a large amount of information about possible disorders of the kidney and lower urinary tract, and systemic disorders that alter urine composition
Results
Color:
Normal Value (Units used in the hospital)
Analysis Interpretation
Yellow
The result has color
Amber
The result is
Yellow
Transparenc y: Slightly turbid
clear 4.8-7.8
SP Gravity:
1.015-1.025
1.020
Sugar:
Negative
There is no pr suga
Negative
There is no pr protei
negative
Protein: +2 RBC: 2.5
Pus cells: 13 Epithelial
0.1/HPF
Indicates no pr infectio 0.2/HPG
Few
cells: few Mucus threads: few
Indicate p Infectio
Few
The kidney is in function.
Nursing Responsibilities for Urinalysis:
BEFORE 1. Check the doctor’s order. 2. Check the right client. 3.
Encourage the SO to increase the fluid intake of the patient.
4. Apply warm on hypogastric region. DURING 1. Provide privacy. 2. Decrease discomfort, and anxiety, allows adequate time. 3. Tell the patient to assume a normal voiding position. 4. Introduce stimuli for voiding. 5. Pour warm water over the perineum. 6. Collect a clean catch urine sample during midstream urination. AFTER 1. Ensure that the specimen label and laboratory requisition form are filled out correctly. 2. Securely attach the label to the container. 3. Send the specimen to the laboratory at once. 4. Document what you have done.
VII. Gordon’s Assessment A.
B.
C.
D.
Health Perception and Management o
Patient can recall being completely immunized
o
Visits a doctor for consultation
o
Takes OTC drugs and herbal medications
Nutrition/Metabolism o
Eats more of fruits and vegetables
o
Eats dried /preserved fish
o
Eats his meals three times a day
o
Allergic to sea foods
Elimination o
Voids usually five times a day
o
Urine color is yellow
o
Defecates usually once a day during morning
Activity/Exercise o
Patient does household chores
o
Able to bathe himself
o
He does simple exercises such as arm exercises by means of shaking and stretching
E.
F.
G.
Sexuality/Reproductive o
Married
o
A father of 3 children
o
No history of STDs
Cognitive/Perceptual o
Oriented to people, time and place
o
Responds to stimuli verbally and physically
o
Able to read and write
o
College graduate
o
In normal thought process
Roles/Relationship o
Married
o
With 3 children
H.
I.
J.
o
Well-ed by the family
o
Loves his family so much
Self –Perception/Self-Concept o
Hopeful to be relieve and treated
o
Manages to practice healthy lifestyle
Value/Belief o
A Roman Catholic
o
Has a strong faith in God
o
Attends Sunday mass
Coping/Stress o
Experienced MVC IN 1995
o
Copes up with problems by talking about it with the family and finds ways to resolve it together
K.
L.
Sleep/Rest o
No difficulties in sleeping
o
Have enough rest intervals
Medication History o
Over the counter medication (buscopan) before issio
VIII. Nursing Care Plans PROBLEM # 1: Decrease cardiac output related to altered heart rate/rhythm ASSESSMENT
S: ø
NURSING
SCIENTIFIC
DIAGNOSIS
EXPLANATION
Decrease cardiac output
Occlusion in the artery
O : The patient
related to altered
Decreased blood
manifested the
heart rate/rhythm
supply
following: Afebrile Conscious and coherent Pale palpebral
Decreased venous return Decreased
conjunctiva
amount of blood
With capillary refill
expelled by ventricles
time of 3 seconds
manifest: Decreased skin turgor Sunken eyeballs Sudden weight loss
Short term:
NURSING INTERVENTIONS 1.
Establish
RATIONALE
1.
EXPECTED OUTCOME
To gain
Short term:
After 1-2 hours of
therapeutic
trust of the
The patient
nursing
relationship
patient
shall have
interventions, the
To note any
participated in
patient will
patient’s
abnormaliti
activities that
participate in
general
es
reduce the
activities that reduce
condition
To have
workload of the
Take and
baseline
heart.
record the
data
the workload of the
2.
3.
heart.
Assess
patient’s vital . 4.
Decreasedcardiac output
The patient may
OBJECTIVES
5.
2.
3.
4.
For comfort
signs
and
Provide
hygiene to
morning care
the patient
Evaluate
5.
To assess
client reports
for signs of
and evidence
poor
of extreme
ventricular
fatigue,
function
intolerance of
and/or
activity and
impending
progressive
cardiac
shortness of
failure
Decreased urine output
breath 6.
Monitor
6.
To note
cardiac
effectivene
Vital signs
rhythm
ss of
taken:
continuously
medication
Decrease
s
T:36.9
7.
RR: 21
stimuli;
HR: 116
provide quiet
7.
adequate
environment
BP: 150/170 8.
9.
Schedule
To promote rest
8.
To
activities and
maximize
assessments
rest periods
Instruct client
9.
Which can
to avoid/limit
cause
activities
changes in
10. ncourage relaxation techniques 11. Provide for
cardiac pressures 10. To reduce anxiety and
diet
conserve
restrictions
energy
12. Encourage
11. To maintain
changing
adequate
positions
nutrition
slowly,
12. To reduce
dangling legs
risk for
before
orthostatic
standing
hypotensio
13. Give information
n 13. To provide
about
encourage
positive signs
ment
of improvement
PROBLEM # 2: Ineffective Peripheral Tissue Perfusion related to decreased cardiac output ASSESSMENT
NURSING
SCIENTIFIC
DIAGNOSIS
EXPLANATION
OBJECTIVES
NURSING INTERVENTIONS
RATIONALE
EXPECTED OUTCOME
S: ø
Ineffective
Ineffective tissue
Short term:
1.
Establish
1.
To build a
Short term:
Peripheral Tissue perfusion is the decrease
After 1-2 hours
therapeutic
good and
O : The patient
Perfusion related
in oxygen resulting in
of nursing
relationship
trusting
shall have
manifested the
to decreased
failure to nourish tissues
interventions,
Assess patient’s
relationship
verbalized
following:
cardiac output
at the capillary level. An
the patient will
general condition
with the
understanding
abrupt increase in
verbalize
Take and record the
patient
of condition,
pressure brings about a
understanding
patient’s vital signs
To assess for
therapy
Vital signs
rapid and reversible
of condition,
that contributes to
complications
regimen, side
taken:
vasoconstriction of small
therapy
the patient’s
To note and
effects of
T:36.9
resistance vessels due to
regimen, side
complaint.
assess for
medications,
RR: 21
their inherent myogenic
effects of
Note current
complicatons
and when to
HR: 116
tone. Prolonged
medications,
situation or
Affecting
BP: 150/170
elevations of pressure
and when to
presence of
systemic
healthcare
can cause a range of
conditions that can
circulation or
provider.
The patient may
more lasting changes in
healthcare
affect perfusion to
perfussion
manifest:
the microcirculation, 2 of
provider.
Hypertension
2.
3.
all body systems
3.
4.
Client at
olyguria
which, remodeling of
capillary refill
small arteries and
conditions
venous
arterioles and rarefaction
associated with
stasis, vessel
of arterioles and
thrombus or emboli
wall injury
Note location of
and
restrictive clothing,
hypercoagula
pressure dressings,
bility
time more than 3 seconds warm extremities
capillaries, will be
4.
2.
5.
considered briefly below.
cyanosis and
edema
higher risk for
circular wraps, cast,
pallor on extremities
Determine history of
6.
5.
That may
or traction device
restrict
Compare skin
circulation to
temperature and
limb. Helps
The patient
paresthesia
7.
color with other limb
differentiate
when assessing
type of
extremity circulation
problems
Assess presence,
6.
location, and degree
identifying or
of swelling or
quantifying
edema formation.
edema in
Measure capillary
involved
time 8.
9. 10. 11. 12.
13. 14.
Useful in
Note client’s
extremity 7.
To determine
nutritional and fluid
adequacy of
status
systemic
Inspect lower extremities for skin texture Palpate arterial pulses Determine pulse equality, as well as intensity Determine time that symptoms are worse, precipitating, or aggravating events Assess motor and sensory function ister medications such as antiplatelet agents, thrombolytics, antibiotics.
circulation 8.
Protein energy malnutrition and weight loss make ischemic tissues more prone to breakdown
9.
That often accompany diminished peripheral perfusion
10. To determine
level of circulatory blockage 11. To evaluate distribution and quality of blood flow, and success or failure of therapy 12. To help isolate and differentiate problems 13. Problems with ambulation; hypersensitivi ty or loss of sensation and numbness and tingling are changes that can indicate neurovascula r dysfunction
14. To improve tissue perfusion or organ function
PROBLEM # 3: Acute Pain as evidence by abdominal pain in the epigastric area secondary to intestinal obstruction
NURSING
SCIENTIFIC
S>O
DIAGNOSIS Acute Pain as
EXPLANATION Intestinal obstruction
O>patient
evidence
refers to a lack of
After 1-2 hours
condition.
manifested:
abdominal
movement
of
of
Monitor
>pain scale of
pain
intestinal
contents
7/10
epigastric area
through the intestine.
patientt will be
>bloatedness
secondary
Because
able to report
> + epigastric
intestinal
smaller
pain
obstruction
obstructions
ASSESSMENT
after
in
by the to
the
of
its
lumen, are
OBJECTIVES Short term:
interventions,
pain
in
epigastric
Vital signs
occur more rapidly in
area.
taken:
the small intestine,
T:36.9
but they can occur in
RR: 21
the large intestine as
BP: 150/170
the
cause
location,
Assess
2.
the
3.
4.
made
of
about
3.
interventio n is more
as soon as it
likely to be
begins
successful
provide comfort
in alleviating
position
-flank pain
example, twisting of
-distraction/
the
guarding
cause sudden total
behaviors
obstruction, whereas
-increased
a
provide
such
pain
of
4.
non-
quiet,
relaxing
pharmacol
environment
ogical pain
6.
5.
encourage
which
-diaphoresis
and discomfort.
activities
-sleep disturbance
7.
to provide adequate
diversional
could lead to pain
to provide
mgmt.
progressive
-pallor
timely
pt to report pain
situation.
obstruction
the
pain. Instruct the
-weakness
elevated BP
be
choices
change
or
info
encourage
gradually developing
PR,RR,
exact
treatment
manifest:
to
shall reported
pain
measures
leads
data
in
acute problem or a
could
the
can
of
rest
like
socialization with
periods
others and slow,
and
rhythmic
prevent
breathing
fatigue
6.
ister analgesics ordered
as
OUTCOME Short term:
baseline
assessment
may
5.
gather
significant
may manifest as an
tumor
a
To
comprehensive
The patient
For
2.
perform
feelings
and
1.
and
verbalization
obstruction
intestine
pt’s
record pt’s VS
decreased
more common and
well. Depending on
1.
EXPECTED
RATIONALE
INTERVENTIONS
nursing
eating
HR: 116
NURSING
to
these could draw the
pt’s
attention away from the pain
patient
decreased flank pain
in
PROBLEM #4: Activity intolerance r/t pain ASSESSMENT s> Ø
NURSING DIAGNOSIS Activity intolerance r/t
o> the patient
EXPLANATION Pain is an unpleasant sensory and emotional
Short term: After 2 hours
NURSING INTERVENTIONS 1. Establish rapport 2. Monitor VS 3. Note patient’s response
of NI, the patient
primarily associated
will identify
with tissue damage or
negative factors
describe in such
affecting activity
as damage, or both
intolerance and
Vital signs taken:
that can be a stressor
eliminate or
and move about and
T:36.9
in performing activities
reduce their
degree of assistance
Pain scale of 7/10 Complaints of pain
RR: 21
of daily living due to
HR: 116
the pain being
BP: 150/170
experienced with certain movements.
The patient may manifest:
OBJECTIVES
experience which I
manifested:
pain
SCIENTIFIC
May acquire risks related with
immobility Further difficulty with
mobility May develop insomnia due to severe pain
effects when possible.
of weakness, fatigue, pain, difficulty accomplishing tasks and/or insomnia 4. Ascertain ability to stand
necessary/use of equipment 5. Provide comfort measures and provide for relief for pain 6. Encourage patient to maintain positive attitude. 7. Instruct patient/SO (s) in monitoring response to activity 8. Plan for progressive increase of activity level, as tolerated by the patient 9. Involve patient/SO (s) in planning of activities
RATIONALE 1. To gain patient and trust and cooperation 2. To obtain baseline data 3. Symptoms may be result of/or contribute to activity intolerance 4. To determine current status and needs associated with participation in needed/desired activities 5. Enhance ability to participate in activities 6. To enhance sense of well being 7. To indicate need to alter activity level 8. Both activity tolerance and health status may improve with progressive
EXPECTED OUTCOME Short term: The patient shall have identified negative factors affecting activity intolerance and eliminate or reduce their effects when possible
PROBLEM #5: Readiness for enhanced knowledge as evidence by expressing interest in learning about disease condition ASSESSMENT
NURSING
SCIENTIFIC
DIAGNOSIS
EXPLANATION
OBJECTIVES
NURSING INTERVENTIONS 1.
S: ø
Establish
RATIONALE 1.
EXPECTED OUTCOME
To build a
Readiness for
The first requirement in
Short term:
therapeutic
good and
Short term:
enhanced
for wellness is a desire
After 1 hour of
relationship
trusting
The patient
O : The patient
knowledge as
to attain a higher level
nursing
Assess patient’s
relationship
shall have
manifested the
evidence by
of well being. The
interventions, the
general condition
with the
verbalized
following:
expressing
patient must express
patient will
patient
understanding
interest in
readiness to engage
verbalize
the patient’s vital
To assess
of information
to health
learning about
and learn interventions
understanding of
signs
for
gained.
teachings
disease
that will help him reach
information
client’s
complicatio
given
condition
that next level.
gained.
level of
ns
Listens intently
2. 3.
4.
Take and record 2.
Assessing a patient’s
knowledge about
knowledge
readiness to respond to
specific topic
assess for
of the topic
wellness diagnosis
Assist client to
complicatio
Explains
5.
involves patient
identify learning
The patient
interviews and
goals
may manifest:
interaction. And
Anxiety Restlessness Fear
To note and
ns 4.
Provides
Ascertain
opportunity
readiness for enhanced
preferred
to ensure
management describes
methods of
accuracy
a patient who is willing
learning
and
Assist client to
completene
in her own treatment by
identify ways to
ss of
following
integrate and use
knowledge
recommendations and
information in all
base for
helping set new goals
appropriate areas
future
and able to participate
6.
3.
7.
for herself.
learning 5.
Helps to frame or focus content to be learned
6.
Identifies best approach to facilitate learning
7.
Ability to apply or use information increases desire to learn and retain information
IX. Drug Study Medical Management IVF’s, BT, NGT feeding, Nebulization, TPN, Oxygen therapy, etc. a. IVF MEDICAL
DATE ORDERED,
MANAGEMENT/
DATE PERFORMED,
TREATMENT
DATE CHANGE
GENERAL
INDICATION OR
DESCRIPTION
PURPOSES
D5LR 1L X 8 HRS
Date ordered: July 2, 2015
For daily maintenance of body fluids and nutrition, and for rehydration.
Treatment for persons needing extra calories who
Date of Results:
cannot tolerate
July 2, 2015
fluid overload.
CLIENT’S RESPONSE TO TREATMENT The patient willingly accepted treatment and is kept hydrated as evidenced by continuous infusion,
Treatment of
improvement in his
shock.
condition and good skin turgor. There were no negative effects noted.
NURSING RESPONSIBILITIES: BEFORE THE PROCEDURE: 1. Assess vital signs for baseline data, skin turgor, bleeding tendencies, disease or 2. 3. 4. 5. 6. 7.
injury to extremities, status of veins to determine appropriate puncture site. Consider: How long the patient is likely to have IV What kinds of fluids will be infused What medications the patient will be receiving or is likely to receive Prepare equipment needed Perform hand hygiene
DURING THE PROCEDURE: 1. Prepare the client: Introduce self and client’s activity 2. Explain the procedure to the client (IV infusion can cause discomfort for a few seconds, but no discomfort while the solution is flowing) 3. Make sure that the client’s clothing or gown can be removed over IV apparatus, if necessary 4. Clean the skin site of entry 5. Assess IV site for any redness, swelling, tenderness, or drainage 6. Ensure appropriate IV flow AFTER THE PROCEDURE: 1. Label the IV with date and time of attachment 2. Document the time of the start of infusion, flow rate, amount and type of solution and client’s general response 3. Teach the client ways to maintain the infusion system 4. Instruct the client to inform any side effects 5. Monitor patient frequently for: 6. 7. 8. 9.
Signs of infiltration/sluggish flow signs of phlebitis/infection well time of catheter and need to be replaced Condition of catheter dressing
10. Check the level of the IVF:
Correct solution, medication, and volume. Check and regulate the drop rate. Change the IVF solution if needed. Do not connect flexible plastic.
b. Drugs
NAME OF
DATE
ROUTE OR
DRUGS,
ORDERED,
ISTRATION
GENERIC
DATE
DOSAGE AND
NAME, BRAND
TAKEN/GIVEN,
FREQUENCY OF
NAME
DATE CHANGED
ISTRATION
GENERAL
CLIENT’S
ACTION,
INDICATION OR
RESPONSE TO
MECHANISM OF
PURPOSES
THE
ACTION
MEDICATION
General action: Generic name:
Date ordered:
OMEPRAZOLE
July 2, 2015
Brand names: LOSEC
Date of Results: July 2, 2015
Antiulcer
It is use to
The patient did
decrease the
not experience
Mechanism of
amount of acid
any adverse
Action:
produced in the
effect.
40 mg TIV O.D.
Inhibits proton pump
PRILOSEC
activity by binding to hydrogenpotassium adenosine triphosphatase, located at secretory surface of gastric parietal cells, to suppress gastric acid secretion. Nursing Responsibilities BEFORE 1. Observe 10 R’s of istration of drugs 2. Check doctor’s order three times and the patient 3. Check the label of the drug, its name and its expiration date 4. Wash hands before handling the medication
stomach
5. Assess patient’s vital signs prior to istering the medication DURING 1. ister as indicated (right drug, right dosage, right frequency) 2. Clean the IV insertion for medication with a cotton ball with alcohol. 3. Gradually inject the drug into the port. Slow IV push to prevent infiltration and phlebitis. 4. ister cautiously and slowly with aseptic technique. AFTER 1. Observe for the sensitivity and side effects to the drug 2. Reassess patient’s level of pain at least 15 and 30 minutes after parenteral istration 3. Monitor circulatory and respiratory status and bladder and bowel function. 4. Caution ambulatory patient about getting out of bed or walking.
NAME OF
DATE ORDERED,
DRUGS,
DATE
GENERIC NAME,
TAKEN/GIVEN,
BRAND NAME
DATE CHANGED
ROUTE OR ISTRATION DOSAGE AND FREQUENCY OF ISTRATION
GENERAL ACTION, MECHANISM OF ACTION
INDICATION OR PURPOSES
Generic name:
Date ordered:
CEFUROXIME
July 2, 2015
Brand names:
Serious lower
Antibiotic
respiratory tract infection, UTI,
Mechanism of
skin or skin-
Action:
structure
CEFTIN,
Inhibits cell-wall
infections, bone
ZINACEF
synthesis,
of t
promoting osmotic
infection,
instability; usually
septicema,
bactericidal.
meningitis and
KEFUROX,
Date of Results:
750 g TIV Q8
General action:
July 2, 2015
gonorrhea - Pharyngitis and tonsillitis - Early lyme disease
Nursing Responsibilities BEFORE 6. Observe 10 R’s of istration of drugs 7. Check doctor’s order three times and the patient 8. Check the label of the drug, its name and its expiration date 9. Wash hands before handling the medication 10. Assess patient’s vital signs prior to istering the medication DURING 5. ister as indicated (right drug, right dosage, right frequency) 6. Clean the IV insertion for medication with a cotton ball with alcohol. 7. Gradually inject the drug into the port. Slow IV push to prevent infiltration and phlebitis. 8. ister cautiously and slowly with aseptic technique. AFTER 5. Observe for the sensitivity and side effects to the drug 6. Reassess patient’s level of pain at least 15 and 30 minutes after parenteral istration 7. Monitor circulatory and respiratory status and bladder and bowel function. 8. Caution ambulatory patient about getting out of bed or walking.
NAME OF DRUGS, GENERIC NAME, BRAND NAME
DATE ORDERED, DATE TAKEN/GIVEN, DATE CHANGED
ROUTE OR ISTRATION DOSAGE AND FREQUENCY OF ISTRATION
GENERAL ACTION, MECHANISM OF ACTION
INDICATION
OR PURPOSE
Generic name: METRONIDAZOLE
Date ordered: July 2, 2015
500 mg TIV Q8
General action:
- Amebic Liver
Antiprotozoal
abscess - Intestinal
Brand names: FLAGYL, FLAGYL
Date of Results: July 2, 2015
Mechanism of
amebiasis
action:
- Trichomonias
ER, FLORAZOLE
Direct acting
ER, NOVO-
trichomonicide and
NIDAZOLE,
amebicide that
FLAGYL IV RTU
works inside and outside the intestines. It's thought to enter the cells of microorganisms that contain nitroreductase. forming unstable compounds that binds to DNA and inhibit synthesis, causing cell death.
Nursing Responsibilities BEFORE 11. Observe 10 R’s of istration of drugs 12. Check doctor’s order three times and the patient 13. Check the label of the drug, its name and its expiration date 14. Wash hands before handling the medication 15. Assess patient’s vital signs prior to istering the medication DURING 9. ister as indicated (right drug, right dosage, right frequency) 10. Clean the IV insertion for medication with a cotton ball with alcohol. 11. Gradually inject the drug into the port. Slow IV push to prevent infiltration and phlebitis. 12. ister cautiously and slowly with aseptic technique. AFTER 9. Observe for the sensitivity and side effects to the drug 10. Reassess patient’s level of pain at least 15 and 30 minutes after parenteral istration 11. Monitor circulatory and respiratory status and bladder and bowel function. 12. Caution ambulatory patient about getting out of bed or walking.
c. Diet TYPE OF DIET
DATE ORDERED,
GENERAL
INDICATION
DATE
DESCRIPTION
SPECIFIC FOOD
CLIENT'S
TAKEN
RESPONSE AND
TAKEN/GIVEN,
REACTION TO
DATE CHANGED
THE DIET NPO
NPO (Nothing per
Date ordered:
Orem)
July 2, 2015
stands
for
Nothing Per Orem
take food or drink
which
through mouth.
means
nothing by mouth. Date of Results: July 2, 2015
Patient cannot
Doctors use this on
orders
when
they do not want the patient to take in any type of food or liquid by mouth. For instance, when a patient is getting ready
for
a
surgery, they are ordered for NPO.
None
Patient cannot eat by mouth thought he can still receive nutrients needed by his body via NGT
Nursing Responsibilities (NPO): Before: Check for the doctor’s order for type of diet preferred. Explain the importance and purpose of the prescribed diet. Place an NPO sign on the bed. Remove all foods at bedside and emphasize strict compliance on the diet regimen. During: Monitor patient closely for compliance of the diet. Reiterate diet frequently to the patient or SO. Check bedside for presence of food, remove if necessary. After: Assess patient’s condition. Document
TYPE OF DIET
NGT
DATE ORDERED,
GENERAL
DATE
DESCRIPTION
INDICATION
SPECIFIC FOOD
CLIENT'S
TAKEN
RESPONSE AND
TAKEN/GIVEN,
REACTION TO
DATE CHANGED
THE DIET
Date ordered: July 2, 2015 Date of Results: July 2, 2015
These are special It It is indicated to preparations for patients who are prevent further unable to digest increase in the solid foods. patient’s blood pressure and to lower down cholesterol levels.
none only
As stated by the
medications
patient, there's a feeling of discomfort.
IX. Health Teachings METHOD M: instructed the patient to take the following Omeprazole Cefuroxime Metronidazole E: Instructed the client to have adequate bed rest T: Instructed the client on strict compliance to medication and therapy H: Instructed patient to always have adequate rest periods in a comfortable position Instructed patient to avoid high fat and high sodium content food Instructed patient to schedule regular follow-up check-up appointments with physician to monitor progress O: Instructed client to continue therapy D: Instructed client on low fat low salt diet
Intestinal Obstruction Partial Probably sec to Colonic Malignancy In Partial Fulfillment of requirements of NCM 107B RLE leading to the degree of Science in Nursing
A Case Study Presented to: Ms. Vanessa O. Umali, R.N. MAN
Presented by: Maria Paula M. Bungay July 26, 2015 TABLE OF CONTENTS
I. Introduction II. Objectives III. Patient’s Profile IV. Anatomy and Physiology V. Pathophysiology VI. Laboratory Examination Results VII. Gordon’s Assessment VIII. Nursing Care Plans IX. Drug Study X. Health Teachings
I. Introduction
2
In the present generation, we cannot deny the reality that different diseases sprout as life progresses. The world is in the generation where diseases are widespread and the medical fields are doing their further research in order to stop them. Being responsible for one’s health is very important for it builds the foundation of a healthy body. It is our choice to live a disease free body. It is always our choice of what food will you eat, how much sleep you need, etc. There are a lot of fashion trends in the world that will make each individual’s life a masterpiece, but the best fashion trend at present is a fit, healthy body. Intestinal obstruction is significant mechanical impairment or complete arrest of the age of contents through the intestine. Symptoms include cramping pain, vomiting, constipation, and lack of flatus. Diagnosis is clinical, confirmed by abdominal x-rays. Treatment is fluid resuscitation, nasogastric suction, and, in most cases of complete obstruction, surgery. According to Bordeianou and Yeh of Wolters Kluwers, Bowel obstruction occurs when the normal flow of intraluminal contents is interrupted. Obstruction can be functional (due to abnormal intestinal physiology) or due to a mechanical obstruction, which can be acute or chronic. Advanced small bowel obstruction leads to bowel dilation and retention of fluid within the lumen proximal to the obstruction, while distal to the obstruction, as luminal contents , the bowel decompresses. If bowel dilation is excessive, or strangulation occurs, perfusion to the intestine can be compromised leading to necrosis or perforation, complications, which increase the mortality, associated with small bowel obstruction. The most common causes of mechanical small bowel obstruction are postoperative adhesions and hernias. Other etiologies of small bowel obstruction include disease intrinsic to the wall of the small intestine (eg, tumors, stricture, intramural hematoma) and processes that cause intraluminal obstruction (eg, intussusception, gallstones, foreign bodies). Acute, mechanical small bowel obstruction is a common surgical emergency. It is estimated that over 300,000 laparotomies per year are performed in the United States for adhesion-related obstructions. Ischemia, which complicates 7 to 42 percent of bowel obstructions, significantly increases mortality associated with bowel obstruction. The small bowel is involved in about 80 percent of cases of mechanical intestinal obstruction. The incidence is similar for males and females. In one Polish study of adult
3
patients, the average age of patients with acute obstruction was 64 years, women comprised 60 percent of the group, and the small bowel was affected in 76 percent. In addition, I have learned and gained new knowledge regarding on Intestinal obstruction. The in-depth understanding of the etiology, pathophysiology, clinical manifestations, diagnosis, treatment and prevention of this condition has yield and enhanced my acquired knowledge. As a student nurse, I also believed that actual interaction with the patient who has the condition being studied can make it easier to understand. Also, to be able to learn completely, one must be able to know how the concepts learned be applied into the actual clinical practice. The knowledge I acquired through this study will give me the opportunity to improve my capability to deliver efficient and appropriate interventions and information to a variety of population. The knowledge, skills and attitude that comprise an effective nurse will be of high regard to promote a reduction in the morbidity and mortality rate. (http://www.uptodate.com/).
II. Objectives Nurse-Centered
4
After the completion of this case study, the nurse will be able to: 1.
Understand the current statistics and latest trend regarding Intestinal Obstruction partial probably sec to Colonic Malignancy.
2.
Describe factually, the personal and pertinent family history of the patient and relate it to the present condition.
3.
Perform comprehensive physical assessment.
4.
Trace the book-based and client-centered pathophysiology of Intestinal Obstruction partial probably sec to Colonic Malignancy.
5.
Determine the predisposing and precipitating factors and the signs and symptoms and relate to the disease process.
6.
Enumerate and describe the diagnostic and laboratory procedures as well as the nursing responsibilities in relation to the disease condition
7.
Enumerate the different treatment modalities and their indication specifically for the patient’s condition.
8.
Identify the pharmacologic treatment provided to the patient, relate the actions of each drug with the disease process and evaluate the patient’s response to the medications given.
9.
Identify nursing diagnoses, formulate short-term goals, carry out appropriate interventions and evaluate the plan.
10. Appraise the effectiveness of medical and surgical nursing management in treating the patient. 11. List the preventive measure for the occurrence of Intestinal Obstruction partial probably sec to Colonic Malignancy for the benefit of the general public. Patient –Centered After the completion of this case study, the patient will be able to: 1. Report understanding of the disease process. 2. Understand the indications of the different diagnostic procedures and medical management involved in her care. 3. Cooperate with the necessary medical and nursing interventions. 4. Adhere with the health teachings provided. 5. Understand the different ways of health promotion and prevention in relation to the disease condition.
5
6. Demonstrate improved conditions as evidenced by absence of further complications. III. Patient’s Profile Name: Mr. Isaw Age: 62 years old Birthday: February 18, 1952 Nationality: Filipino Religion: Roman Catholic Civil Status: Married Date ission: July 2, 2015 Time of ission: 12:15 PM Chief Complaint's: Abdominal Pain Initial Diagnosis: Intestinal Obstruction Partial Probably sec to Colonic Malignancy Final Diagnosis: None
HISTORY OF PAST ILLNESS During the previous years, Mr. Isaw was diagnosed Hypertensive in 2014 and a history of vehicular accident 20 years ago, which affected his Left femur. He is a non-smoker and non-alcoholic. As for childhood illness, he had chicken pox and measles. He also experienced coughs and colds for common illness. To relieve symptoms, he would take different herbal plants or purchase over-the-counter drugs. For the herbal plants, he prepares decoction with one to two glasses of water for fifteen minutes or until one half of the liquid is left. Then, he will drink it. He also experienced fever once in a while in which he takes over-the-counter drugs. Mr. Isaw, has no family history of hypertension, Diabetes, Arthymias, Pulpomonary Tuberculosis, and Cancer. For food allergies, crab and shrimp are contraindicated but no allergies to drugs. HISTORY OF PRESENT ILLNESS Prior to ission, Mr. Isaw complained of sudden onset abdominal pain described as bloatedness more prominent in the epigastric and right periumbilical area. There was no
6
associated nausea, vomiting, change in bowel habits, hematochezia, melena, jaundice and fever. Patient consulted at PGH, Abdominal X-ray revealed dilated small bowels. He was then referred to the institution for further management. PHYSICAL ASSESSMENT Physician’s Physical Assessment done by the Resident on Duty (July 2, 2015, lifted from the patient's chart) Height: 5’6 Weight: 81 kg Vital Signs as follows: T: 36.9 °C
PR: 116 bpm
RR: 18m
BP: 150/90 mmHg
SAO2: 97%
GENERAL SURVEY Mr. Isaw, Assessed/received patient lying on bed, awake, conscious, responsive, and coherent. With the following vital signs: Temperature: 36.7 °C Heart rate: 70 bpm Respiratory rate: 20 bpm Blood Pressure: 140/90 mmHg SAO2: 96% NUTRITIONAL STATUS Upon ission, Mr. Isaw was placed on NPO and IVF of D5LR 1 x Q8. CBC, BT, PTPTT, FBS, BUN, CREA, Na, K, Cl, 12-LECG, Chest X-ray PA, abdominal series, and Urinalysis were requested. NGT and Foley Catheter were inserted.
SKIN
7
> Pallor noted. > Good skin turgor in both upper and lower extremities; the skin returns to its previous state immediately after being tented. > warm moist skin, no active dermatoses. HAIR > Hair is black and is evenly distributed. > Silky and smooth hair. > No areas of hair loss noted. > Thick hair strands. NAILS > Trimmed clean nails. > Concave shaped; with a nail plate angle of about 160 degrees. > Smooth in texture. > Intact epidermal lining around the nails. > Capillary Refill Test less than 3 seconds. SKULL AND FACE > Rounded (normocephalic and symmetrical with frontal, parietal and occipital prominences). > Head has no cervical lymphadenophaties > No nodules or masses upon palpation. EYES AND VISION
8
> Eyebrows and eyelashes are evenly distributed. > Eyelids are intact > Pink palpebral conjuctiva > Sclera appears white. > Pale conjunctiva. > No discharges and discoloration noted. > Blink reflex intact. EARS AND HEARING > Ears are symmetrical in size and in line with the outer canthus of the eyes. > Color of ears is the same with the facial skin. > No discharges and foul odor noted upon inspection. > Pinna and ear canal are clean. > Auricles are firm and recoil to previous state when folded. > No nodules or masses noted upon palpation NOSE AND SINUSES > No nasal discharge > No tenderness masses and pain noted upon palpation OROPHARYNX (Mouth and Throat) > Dry and pale lips noted upon inspection > Tongue is able to move freely
9
> Good oral hygiene. > Thyroid gland moves with deglutition NECK > Jugular vein is not visible > Muscles are equal in size with the head centered > Slow muscle movement > Lymph nodes are not palpable CARDIOVASCULAR AND PERIPHERAL SYSTEM > Skin color of palm of the hand and feet is pink. > Pink nail beds upon inspection. > Symmetric pulse volumes, full pulsations of peripheral pulses. > Heart rate is 70 beats per minute. > Blood Pressure is 140/90 mmHg > (Vital signs taken during the time of assessment July 2, 2015 at 0715H) RESPIRATORY SYSTEM > + DOB > Symmetric chest expansion > Skin and chest wall are intact and has uniform temperature > No tenderness and masses noted upon palpation > Regular breathing pattern
10
> Presence wheezing and crackles sound upon auscultation > Full and symmetric chest wall expansion BREAST AND AXILLAE > Breasts are symmetrical in size; color is the same as with the abdomen. > Both nipples are symmetrical in size. > No discharges noted. > No tenderness, masses, and nodules noted upon palpation. ABDOMEN > Direct tenderness at epigastric area. > Abdominal skin is intact. > Distended abdomen noted. > Audible bowel sound upon auscultation. > Abdominal dullness upon percussion. MUSCULOSKELETAL > Posture is good, able to stand straight and can walk alone properly but slowly > Scar at left thigh and right medial leg and foot NEUROLOGIC >with a GCS of 15 > Patient has times of looking in the distance and is slow in response when a question asked.
11
> Patient was able to answer well when asked of her complete name, birth date and age. URINARY SYSTEM > Patient has indwelling Foley Catheter REPRODUCTIVE SYSTEM > The patient refused to be assessed with her external reproductive organ but she verbalized that she has minimal vaginal bleeding and complain of pain when secretions are expelled. REVIEW OF SYSTEM Integumentary System The patient has no history of bruises in both upper and lower extremities. Head The patient had no history of any form of head injuries. Eyes Patient had no history of any eye problems. Ears and Hearing Patient had no history of smelly discharges on both ears, and no complaints of hearing impairment. Breast and Axillae The patient had no history of breast nodules, no enlargement, no tenderness, no pain and unusual discharges. Respiratory System
12
The patient has no history of asthma or other respiratory problems. Cardiovascular System The patient has a history of hypertension. Genitourinary System The patient had no history of any genital problems. Usually urinates 5 times a day. Gastrointestinal System The patient had experienced abdominal pain. Musculoskeletal System Patient has no history of t pain. Neurologic System Patient had no history of any major mental problems.
Cranial Nerve Assessment:
13
CRANIAL NERVE
ASSESSMENT TECHNIQUE
EXPECTED OUTCOME
ACTUAL FINDINGS
I: Olfactory Type: Sensory Function: Smell
Ask the client to identify a scented object that you are holding.
Client is able to identify different smell with each nostril separately and with eyes closed unless such condition like colds is present.
The client was able to identify the aromas of cologne and alcohol that she had smelled.
II: Optic Type: Sensory Function: Vision
Provide adequate lighting and ask client to read words on a newspaper held at a distance of 36 cm (14 inches) with each eye first then both eyes.
The client should be able to read with each eye and both eyes.
The client was able to read the words in the newspaper at 14 inches.
III: Oculomotor, IV: Trochlear & VI: Abducens Type: Motor Function: Upward and Downward movement of Pupils.
-Hold a penlight 1 ft. -Client’s eyes should in front of the client’s be able to follow the eyes. Ask the client to penlight as it moves. follow the movements of the penlight with the eyes only. Move the penlight upward, downward, sideward and diagonally. -Ask the client to look straight ahead then approach the pupil with a penlight and observe for pupil constriction.
-The client’s eyes will have a normal reaction for PERRLA.
-Both eyes of the client were able to follow the Penlight’s movements.
-The client had a normal reaction to PERRLA as Pupils are equally round, reactive to light and accommodation.
V: Trigeminal Type: Sensory Function: Sensation of cornea
While client looks upward, lightly touch the lateral sclera of eye to elicit blink reflex.
Client should have a positive corneal reflex.
The client was able to elicit corneal reflex.
VII: Facial Type: Motor Function: Facial movements
Ask client to: smile, frown and wrinkle forehead, show teeth, puff out cheeks,
Client should smile, frown and wrinkle forehead, show teeth, puff out cheeks,
The client was able to do the facial movements symmetrically.
14
purse lips, raise eyebrows, close eyes tightly against resistance
purse lips, raise eyebrows, close eyes tightly against resistance. Movements are symmetrical.
VIII: Vestibulocochlear/ acoustics Type: Sensory Function: Hearing
Have the Client occlude one ear. Out of the client’s sight, place a tickling watch 2 cm. Ask what the client can hear and repeat with the other ear.
Client should be able to hear the ticking of the watch in both ears.
The client was able to hear the ticking of the watch in both ears.
IX. Glossopharyngeal & X: Vagus Type: Motor Function: Swallowing and Speaking
Ask the client to swallow and say its name.
The client should be able to swallow without difficulty and speak audibly.
The client was able to swallow without difficulty and speak audibly.
XI. Spinal Accessory Type: Motor Function: strength and resistance
-Ask client to shrug the shoulders against your hands.
-There is symmetric, strong contraction of the trapezious muscles.
The client was able to symmetrically contract the trapezious muscle.
-Ask client to turn the head against resistance, first to the right then to the left, to assess the sternocleidomastoid muscle.
-There is strong contraction of the sternocleidomastoid muscle on the side opposite to the turned face.
-The client was able to contract strenocleidomastoid muscleon the side opposite to the turned face.
Ask the client to protrude the tongue and move in different directions.
The client will be able to protrude her tongue and move in different directions.
The client was able to protrude his tongue and move it in different directions.
XII: Hypoglossal Type: Motor Function: Movement and strength of tongue
15
IV. Anatomy and Physiology The digestive system, sometimes called the gastrointestinal tract, alimentary tract, or gut, consists of a long hollow tube which extends through the trunk of the body, and its accessory structures: the salivary glands, liver, gallbladder, and pancreas. The digestive tract is divided into two sections, the upper tract, consisting of the mouth, esophagus, and stomach, and the lower tract, consisting of the intestines. FIGURE 20-1 Anatomy of the digestive system with associated events.
Inside this tube, ingested food and fluid, along with secretions from various glands, are efficiently processed. First, they are broken down into their separate constituents; then the desired nutrients, water, and electrolytes are absorbed into the blood for use by the cells, and waste elements are eliminated from the body. Within this system, the liver can reassemble the
component nutrients into new materials as they are needed by the body. For example, the proteins in milk are digested by enzymes in the digestive tract, producing the component amino acids, which are then absorbed into the blood. The individual amino acids are used by the liver cells to produce new proteins, such as albumin or prothrombin, or they may circulate as they are in the amino acid pool in the blood to be taken up by individual cells as necessary. The peritoneal cavity refers to the potential space between the parietal and visceral peritoneum. A small amount of serous fluid is present in the cavity to facilitate the necessary movement of structures such as the stomach. Numerous lymphatic channels drain excessive fluid from the cavity. Because serous membranes are normally thin, somewhat permeable, and highly vascular, the peritoneal membranes are useful as an exchange site for blood during peritoneal dialysis in patients with kidney failure. However, such an extensive membrane may also facilitate the spread of infection or malignant tumor cells throughout the abdominal cavity or into the general circulation. The mesentery is a double layer of peritoneum that s the intestines and conveys blood vessels and nerves to supply the wall of the intestine. The mesentery attaches the jejunum and ileum to the posterior (dorsal) abdominal wall. This arrangement provides a balance between the need for of the intestines and the need for considerable flexibility to accommodate peristalsis and varying amounts of content. The greater omentum is a layer of fatty peritoneum that hangs from the stomach like an apron over the anterior surface of the transverse colon and the small intestine. The lesser omen-tum is part of the peritoneum that suspends the stomach and duodenum from the liver. When inflammation develops in the intestinal wall, the greater omentum, with its many lymph nodes, tends to adhere to the site, walling off the inflammation and temporarily localizing the source of the problem. Inflammation of the omentum and peritoneum may lead to scar tissue and the formation of adhesions between structures in the abdominal cavity, such as loops of intestine, restricting motility and perhaps leading to obstruction. Intestinal Obstruction Intestinal obstruction refers to a lack of movement of the intestinal contents through the intestine. Because of its smaller lumen, obstructions are more common and occur more rapidly in the small intestine, but they can occur in the large intestine as well. Depending on the cause and location, obstruction may manifest as an acute problem or a gradually developing situation. For example, twisting of the intestine could cause sudden total obstruction, whereas
a tumor leads to progressive obstruction. FIGURE 20-37 Colostomy. A, sigmoid colostomy-a surgically created opening into the colon through the abdominal wall. B, The stoma is the new opening on the abdomen. It is always red and moist, is not painful, but may bleed easily. C, A plastic pouch to collect stools is attached to the stoma. (Courtesy of Hollister Incorporated, Patient Education Series.)
Intestinal obstruction occurs in two forms. Mechanical obstructions are those resulting from tumor, adhesions, hernias, or other tangible obstructions. Functional, or adynamic, obstructions result from neurologic impairment, such as spinal cord injury or lack of propulsion in the intestine, and are often referred to as paralytic ileus. While the end result can be the same, these types manifest somewhat differently and require different treatment.
Colon The colon is the last part of the digestive system in most vertebrates; it extracts water and salt from solid wastes before they are eliminated from the body, and is the site in which flora-aided (largely bacteria) fermentation of unabsorbed material occurs. Unlike the small intestine, the colon does not play a major role in absorption of foods and nutrients. However, the colon does absorb water, potassium and some fat soluble vitamins. In mammals, the colon consists of four sections: the ascending colon, the transverse colon, the descending colon, and the sigmoid colon (the proximal colon usually refers to the ascending colon and transverse colon). The colon, cecum, and rectum make up the large intestine. The location of the parts of the colon are either in the abdominal cavity or behind it
in
the retroperitoneum. The colon in those areas is fixed in location. Arterial supply to the colon comes from branches of the superior mesenteric artery (SMA) and inferior mesenteric artery (IMA). Flow between these two systems communicates via a "marginal artery" that runs parallel to the colon for its entire length. Historically, it has been believed that the arc of Riolan, or the meandering mesenteric artery (of Moskowitz), is a variable vessel connecting the proximal SMA to the proximal IMA that can be extremely
important if either vessel is occluded. However, recent studies conducted with improved imaging technology have questioned the actual existence of this vessel, with some experts calling for the abolition of the from future medical literature. Venous drainage usually mirrors colonic arterial supply, with the inferior mesenteric vein draining into the splenic vein, and the superior mesenteric vein ing the splenic vein to form the hepatic portal vein that then enters the liver. Lymphatic drainage from the entire colon and proximal two-thirds of the rectum is to the paraaortic lymph nodes that then drain into the cisterna chyli. The lymph from the remaining rectum and anus can either follow the same route, or drain to the internal iliac and superficial inguinal nodes. The pectinate line only roughly marks this transition. Ascending colon The ascending colon, on the right side of the abdomen, is about 25 cm long in humans. It is the part of the colon from the cecum to the hepatic flexure (the turn of the colon by the liver). It is secondarily retroperitoneal in most humans. In ruminant grazing animals, the cecum empties into the spiral colon. Anteriorly it is related to the coils of small intestine, the right edge of the greater omentum, and the anterior abdominal wall. Posteriorly, it is related to the iliacus, the iliolumbar ligament, the quadratus lumborum, the transverse abdominis, the diaphragm at the tip of the last rib; the lateral cutaneous, ilioinguinal, and iliohypogastric nerves; the iliac branches of the iliolumbar vessels, the fourth lumbar artery, and the right kidney. The ascending colon is supplied by parasympathetic fibers of the vagus nerve (CN X). Arterial supply of the ascending colon comes from the ileocolic artery and right colic artery, both branches of the SMA. While the ileocolic artery is almost always present, the right colic may be absent in 5–15% of individuals. Transverse colon The transverse colon is the part of the colon from the hepatic flexure to the splenic flexure (the turn of the colon by the spleen). The transverse colon hangs off the stomach, attached to it by a wide band of tissue called the greater omentum. On the posterior side, the transverse colon is connected to the posterior abdominal wall by a mesentery known as the transverse mesocolon. The transverse colon is encased in peritoneum, and is therefore mobile (unlike the parts of the colon immediately before and after it). Cancers form more frequently further along the large intestine as the contents become more solid (water is removed) in order to form feces. The proximal two-thirds of the transverse colon is perfused by the middle colic artery, a branch of SMA, while the latter third is supplied by branches of the IMA. The "watershed" area
between these two blood supplies, which represents the embryologic division between the midgut and hindgut, is an area sensitive to ischemia. Descending colon The descending colon is the part of the colon from the splenic flexure to the beginning of the sigmoid colon. The function of the descending colon in the digestive system is to store food that will be emptied into the rectum. It is retroperitoneal in two-thirds of humans. In the other third, it has a (usually short) mesentery. The arterial supply comes via the left colic artery. Sigmoid colon The sigmoid colon is the part of the large intestine after the descending colon and before the rectum. The name sigmoid means S-shaped (see sigmoid). The walls of the sigmoid colon are muscular, and contract to increase the pressure inside the colon, causing the stool to move into the rectum. The sigmoid colon is supplied with blood from several branches (usually between 2 and 6) of the sigmoid arteries, a branch of the IMA. The IMA terminates as the superior rectal artery. Sigmoidoscopy is a common diagnostic technique used to examine the sigmoid colon. Redundant colon One variation on the normal anatomy of the colon occurs when extra loops form, resulting in a longer than normal organ. This condition, referred to as redundant colon, typically has no direct major health consequences, though rarely volvulus occurs resulting in obstruction and requiring immediate medical attention.[4] A significant indirect health consequence is that use of a standard adult colonoscope is difficult and in some cases impossible when a redundant colon is present, though specialized variants on the instrument (including the pediatric variant) are useful in overcoming this problem. Standing gradient osmosis Water absorption at the colon typically proceeds against a transmucosal osmotic pressure gradient. The standing gradient osmosis is a term used to describe the reabsorption of water against the osmotic gradient in the intestines. This hypertonic fluid creates an osmotic pressure that drives water into the lateral intercellular spaces by osmosis via tight junctions and adjacent cells, which then in turn moves across the basement membrane and into the capillaries. Functions of the Colon
There are differences in the large intestine between different organisms, the large intestine is mainly responsible for storing waste, reclaiming water, maintaining the water balance, absorbing some vitamins, such as vitamin K, and providing a location for flora-aided fermentation.Vitamin K is essential as a coagulation factor. By the time the chyme has reached this tube, most nutrients and 90% of the water have been absorbed by the body. At this point some electrolytes like sodium, magnesium, and chloride are left as well as indigestible parts of ingested food (e.g., a large part of ingested amylose, protein which has been shielded from digestion heretofore, and dietary fiber, which is largely indigestible carbohydrate in either soluble or insoluble form). As the chyme moves through the large intestine, most of the remaining water is removed, while the chyme is mixed with mucus and bacteria (known as gut flora), and becomes feces. The ascending colon receives fecal material as a liquid. The muscles of the colon then move the watery waste material forward and slowly absorb all the excess water. The stools get to become semi solid as they move along into the descending colon. The bacteria break down some of the fiber for their own nourishment and create acetate, propionate, and butyrate as waste products, which in turn are used by the cell lining of the colon for nourishment. No protein is made available. In humans, perhaps 10% of the undigested carbohydrate thus becomes available; in other animals, including other apes and primates, who have proportionally larger colons, more is made available, thus permitting a higher portion of plant material in the diet. This is an example of a symbiotic relationship and provides about one hundred calories a day to the body. The large intestine produces no digestive enzymes -— chemical digestion is completed in the small intestine before the chyme reaches the large intestine. The pH in the colon varies between 5.5 and 7 (slightly acidic to neutral).
Colonic Carcinoma / Colon Carcinoma / Colon Cancer Definition: It is a disease in which malignant (cancer) cells form in the tissues of the colon. The colon is part of the body's digestive system. The digestive system removes and processes nutrients (vitamins, minerals, carbohydrates, fats, proteins, and water) from foods and helps waste material out of the body. The digestive system is made up of the esophagus, stomach, and the small and large intestines. The first 6 feet of the large intestine are called the large bowel or colon. The last 6 inches are the rectum and the anal canal. The anal canal ends at the anus (the opening of the large intestine to the outside of the body). Risk Factors: Age and health history can affect the risk of developing colon carcinoma . Risk factors include the following:
Age 50 or older.
A family history of carcinoma of the colon or rectum.
A personal history of carcinoma of the colon, rectum, ovary, endometrium, or breast.
A history of polyps in the colon.
Signs and Symptoms:
A change in bowel habits.
Blood (either bright red or very dark) in the stool.
Diarrhea, constipation, or feeling that the bowel does not empty completely.
Stools that is narrower than usual.
Frequent gas pains, bloating, fullness, or cramps.
Weight loss for no known reason.
Feeling very tired.
Vomiting. A specimen removed from a patient with colonic carcinoma
V. Pathophysiology Pathophysiology of Intestinal obstruction
Risk Factors for Intestinal obstruction
Crohn’s disease – narrows intestinal ageways due to thickening Abdominal Cancer
2 types of obstructions
Mechanical: (+) Physical obstruction or increased pressure from walls creating a blockage
(+) Increased fluid and gas
Functional: Intestinal muscles cannot propel the contents along the bowel
Increased pressure on intestinal wall causes more fluid to enter intestine
(+) Severe vomiting & pain
(+) Dehydration & Electrolyte Imbalance
Decreased blood pressure &pressure on Continued hypovolemic shock intestinal wall causes edema, ischemia and decreased peristalsis
(+) Increased peristalsis attempts to force contents past obstruction
(+) Abdominal distention
Prolonged ischemia causes increased permeability and necrosis of wall. Intestinal bacteria & toxins leak into blood.
(+) mass in the small intestine
Pathophysiology of Colon Cancer
Predisposing factors: (+) Age (56% >70yrs old) Colorectal polyps Family history Previous colorectal cancer Ulcerative colitis /colonic crohn’s disease
Diagnostic test: Fecal occult blood test SigmoIdoscopy Digital Rectum Exam
Surgical Treatment: Colonoscopy Virtual Colonoscopy
Precipitating factors: Patient broke her right leg due to falling on the stairs Precipitating factors: Diet – high fat/low fiber Smoking Alcohol drinking (+)Lack of exercise
Etiology: Unknown
Abnormal proliferation of cells in the colon area
Signs and Symptoms: Rectal bleeding Bloody stools (+) Abdominal pain (+) Fatigue Constipation (+)Diarrhea
Arising from epithelial lining of the intestine
Benign polyps occur
(+) Nausea and Vomiting
Continuous plorifetation of cells in the polyps
Polypectomy Reduction likelihood of regrowth
Increase in size of the polyps
Exposure to carcinogens
Development of malignant tumor
Uncontrolled Increase in proliferation COLON CANCER size of cells in the tumor
Complications DEATH occur
Diagnostic test: SigmoIdos copy
VI.
Laboratory Examination
Results Diagnostic/ Laboratory Procedures
Date ordered Date results in
1. Complete Blood Count
Indications or Purposes
Results
Normal Value (Units used in the hospital)
Analysis and Interpretation of results
Hgb: 153
N: 115-175 g/L
The hemoglobin level is normal. This indicates that RBC is capable of carrying O2 and CO2 throughout the body.
Hct: 0.44
N: 0.40-0.52
The result indicates there is normal concentration of RBC within the blood
CBC is a screening test, used to diagnose and manage numerous diseases. The results can reflect problems with fluid or loss of blood.
a. Hemoglobin
Date ordered/ Date of Results: July 2, 2015
b. Hematocrit
Date ordered/ Date of Results: July 2, 2015
Hemoglobin determines the RBC that carries oxygen and carbon dioxide throughout the body
Hematocrit determines the
concentration of RBC within the blood volume c. RBC Date ordered/ Date of Results: July 2, 2015
volume.
RBC: 4.93
N:4.5-6.2
The result is within normal range which indicates that the body's RBCs containing hemoglobin, carrying oxygen to the body's tissues are functioning normally.
WBC: 13.0
N: 5-10x 109/L
WBC is high which indicates that there is infection presented in the body.
An RBC count is a blood test that measures how many red blood cells (RBCs) you have. RBCs contain hemoglobin, which carries oxygen. How much oxygen your body tissues get depends on how many RBCs you have and how well they work.
d. WBC Date ordered/ Date of Results: July 2, 2015
White blood cells (WBCs), also called leukocytes, are an important part of the immune system. These cells help
fight infections by attacking bacteria, viruses, and germs that invade the body. White blood cells originate in the bone marrow, but circulate throughout the bloodstream.
DIFFERENTIAL COUNT
a. Segmenters Segmenters: 0.84 Date ordered/ Date of Results: July 2, 2015
A type of white blood cell that respond to bacterial infections. Where the blood count has high levels of segmenters, this indicates the presence of a bacterial infection. Where there is a low level of segmenters, the patient is likely to be suffering from a viral infection or
N: 0.55-0.65
The result is higher than the normal range. Which indicates presence of bacterial infection.
an autoimmune disease.
b.Lymphocytes
Lymphocytes: 0.27 Date ordered/ Date of Results: July 2, 2015
Lymphocytes are responsible for immune responses. There are two main types of lymphocytes: B cells and T cells. The B cells make antibodies that attack bacteria and toxins while the T cells attack body cells themselves when they have been taken over by viruses or have become cancerous. Lymphocytes secrete products (lymphokines) that modulate the functional activities of many other types of cells and are often present at sites of chronic inflammation.
N: 0.25-0.35
Normal count of lymphocytes indicates that there is no presence of infection in the body
c. Eosinophils
N: 0.02-0.04 0.00 Date ordered/ Date of Results: July 2, 2015
Eosinophils are a specific type of white blood cell that protects your body against certain kinds of germs, mainly bacteria and parasites. They're also what causes you to have allergic reactions.
d. Monocytes Date ordered/ Date of Results: July 2, 2015
The result is below the normal range. Which indicates no significant.
0.06 Monocytes are a type of white blood cell that fights off bacteria, viruses and fungi. Monocytes are the biggest type of white blood cell in the immune system. Originally formed in the bone marrow, they are released into our blood and tissues. When certain germs enter the body, they quickly rush
N: 0.03-0.06
The result is normal. Which indicates that the body can fights off bacteria, virus and fungi,
to the attack.
site
for
e. Basophils Date ordered/ Date of Results: July 2, 2015
N: 0.00-0.01
Platelet Count: 311
Platelet Count: 150- 400 x 109/L
Basophils are granulocytic white blood cells that are active in the inflammatory response. They are mostly found in the skin and mucosa tissues, which are the tissues lining the openings into the body. They represent about 1% of all white blood cells in the body.
Platelet Count Date ordered/ Date of Results: July 2, 2015
0.00
A platelet count is a test to measure how many platelets you have in your blood. Platelets are parts of the blood that help the blood clot. They are smaller than red
The result is normal, which indicates that body is active for inflammatory response.
The result is within the normal range indicates that there is enough platelet produces for coagulation.
or white cells.
blood
Nursing Responsibilities: BEFORE 1. Explain to the patient the procedure and its purposes. 2. If the patient has eaten a meal with high sodium content in the past 24 hours, this should be noted. 3. Be sure not to draw blood, which has infused IVF. 4. Note if patient’s on a diet that restricts sodium and other nutrients. 5. Note other conditions such as diabetes. 6. Carefully watch for signs of electrolyte imbalance. 7. Perform a complete cephalocaudal assessment especially cardiac assessment and vital signs. 8. Make sure to have the right patient, specimen and method. DURING 1. Clean injection site with alcohol. 2. Lower the patient’s arm to dilate the veins. 3. Apply tourniquet and ask the patient to open and close fist. 4. Remove the tourniquet when drawing the final tube of blood. AFTER 1. Note for any signs of discomfort or bruising at the puncture site. 2. Provide pressure at the puncture site to stop bleeding and reduce bruising. 3. Apply warm compress to puncture site to relieve discomfort. 4. Send the specimen at the laboratory.
B. Blood Chemistry Diagnostic/ Laboratory Procedures
Date ordered Date results in
Indications or Purposes
Date ordered:
A serum creatinine test — which measures the level of creatinine in your blood — can indicate whether your kidneys are working properly.
70.10 umol/L
It regulates body water along with potassium. It is responsible for nerve conduction and contraction of muscle.
Na: 141
Results
Normal Value (Units used in the hospital)
Analysis and Interpretation of results
2. CLINICAL CHEMISTRY TEST
Creatinine
July 2, 2015 Date of Results: July 2, 2015
Sodium
Date ordered: July 2, 2015 Date of Results: July 2, 2015
N: 71-115 umol/L
The result is lower than the normal range which indicate that the kidney has a slightlyl glomerular filtration and renal damage. Creatinine is more accurate for renal condition.
N: 135-148 mmol/L
The result is within normal range, it indicates no presence of hypernatremia or hyponatremia
Potassium
Date ordered: July 2, 2015 Date of Results: July 2, 2015
Chloride
Date ordered: July 2, 2015 Date of Results: July 2, 2015
It is a mineral, which with Sodium and Calcium maintains normal heart rhythm and regulates water balance. A chloride test measures the level of chloride in your blood or urine. Chloride is one of the most important electrolytes in the blood. It helps keep the amount of fluid inside and outside of your cells in balance. It also helps maintain proper blood volume, blood pressure, and pH of your body fluids. Tests for sodium, potassium, and bicarbonate are usually done at the same time as a blood test for chloride.
K: 4.10
104.4
N: 3.5-5.3 mmol/L
N: 98-107 mmol/L
The result is within normal range, which indicates no presence of hyperkalemia or hypokalemia
The result is within normal range, which indicates there is normal functioning of the muscles, heart, and nerves. Which is also essential for normal fluid absorption and excretion.
Alanine Aminotrans liquid
Date ordered: July 2, 2015 Date of Results: July 2, 2015
Aspartate Aminotrans liquid
Date ordered: July 2, 2015 Date of Results: July 2, 2015
The blood test for aspartate aminotransferase (AST) and alanine aminotransferase (ALT) are usually used to detect liver damage. It is often ordered to screen for and/or help diagnose liver disorders. In the patient’s case, liver function is monitored due to metastasis of his cancer to his liver. The blood test for aspartate aminotransferase (AST) and alanine aminotransferase (ALT) are usually used to detect liver damage. It is often ordered to screen for and/or help diagnose liver disorders. In the patient’s case, liver function is monitored due to metastasis of his cancer to his liver.
19.0 U/L
18.6 U/L
N:10.0-44.0
N: 10.0-34.0
The result is within the normal range. Which indicates that liver is functioning normally.
The result is within the normal range. Which indicates that liver is functioning normally.
Calcium Gen 2
Date ordered: July 2, 2015 Date of Results: July 2, 2015
The Calcium Gen.2 assay is an in vitro diagnostics reagent system intended for the quantitative determination of calcium in human serum, plasma, and urine on Roche/Hitachi cobas c systems. Calcium measurements are used in the diagnosis and treatment of parathyroid disease, a variety of bone diseases, chronic renal disease, and tetany.
2.18 mmol/L
N: 2.20-2.75
The result is within the normal range.
NURSING RESPONSIBILITIES BEFORE 1. Confirm the patient’s identity using two patient identifiers according to facility policy. 2. Explain the procedure and the indication. 3. Inform the patient that the test requires blood sample, and explain that he may experience slight discomfort from the tourniquet and the needle puncture. 4. Instruct the patient that he doesn’t need to restrict food and fluids. For triglycerides she should not eat 12 hours before procedure. 5. Notify the laboratory and practitioner about any medications the patient is taking that may affect test results; they may need to be restricted. DURING 1. Perform venipuncture and collect the sample in a 3- or 4-mL clot activator tube. 2. Handle sample gently to prevent hemolysis. AFTER 1. A report of the results will be sent to the requesting Health Care Provider, who will discuss the results with the patient. 2. Depending on the results of this procedure, additional testing may be performed to evaluate or monitor progression of the disease process and determine the need for a change in therapy. 3. Evaluate test results in relation to the patient's symptoms and other tests performed.
Diagnostic/ Laboratory Procedures
Date ordered Date results in
2. Urinalysis
Date ordered: July 2, 2015 Date of Results: July 2, 2015
Indications or Purposes
Urinalysis yields a large amount of information about possible disorders of the kidney and lower urinary tract, and systemic disorders that alter urine composition
Results
Color:
Normal Value (Units used in the hospital)
Analysis Interpretation
Yellow
The result has color
Amber
The result is
Yellow
Transparenc y: Slightly turbid
clear 4.8-7.8
SP Gravity:
1.015-1.025
1.020
Sugar:
Negative
There is no pr suga
Negative
There is no pr protei
negative
Protein: +2 RBC: 2.5
Pus cells: 13 Epithelial
0.1/HPF
Indicates no pr infectio 0.2/HPG
Few
cells: few Mucus threads: few
Indicate p Infectio
Few
The kidney is in function.
Nursing Responsibilities for Urinalysis:
BEFORE 1. Check the doctor’s order. 2. Check the right client. 3.
Encourage the SO to increase the fluid intake of the patient.
4. Apply warm on hypogastric region. DURING 1. Provide privacy. 2. Decrease discomfort, and anxiety, allows adequate time. 3. Tell the patient to assume a normal voiding position. 4. Introduce stimuli for voiding. 5. Pour warm water over the perineum. 6. Collect a clean catch urine sample during midstream urination. AFTER 1. Ensure that the specimen label and laboratory requisition form are filled out correctly. 2. Securely attach the label to the container. 3. Send the specimen to the laboratory at once. 4. Document what you have done.
VII. Gordon’s Assessment A.
B.
C.
D.
Health Perception and Management o
Patient can recall being completely immunized
o
Visits a doctor for consultation
o
Takes OTC drugs and herbal medications
Nutrition/Metabolism o
Eats more of fruits and vegetables
o
Eats dried /preserved fish
o
Eats his meals three times a day
o
Allergic to sea foods
Elimination o
Voids usually five times a day
o
Urine color is yellow
o
Defecates usually once a day during morning
Activity/Exercise o
Patient does household chores
o
Able to bathe himself
o
He does simple exercises such as arm exercises by means of shaking and stretching
E.
F.
G.
Sexuality/Reproductive o
Married
o
A father of 3 children
o
No history of STDs
Cognitive/Perceptual o
Oriented to people, time and place
o
Responds to stimuli verbally and physically
o
Able to read and write
o
College graduate
o
In normal thought process
Roles/Relationship o
Married
o
With 3 children
H.
I.
J.
o
Well-ed by the family
o
Loves his family so much
Self –Perception/Self-Concept o
Hopeful to be relieve and treated
o
Manages to practice healthy lifestyle
Value/Belief o
A Roman Catholic
o
Has a strong faith in God
o
Attends Sunday mass
Coping/Stress o
Experienced MVC IN 1995
o
Copes up with problems by talking about it with the family and finds ways to resolve it together
K.
L.
Sleep/Rest o
No difficulties in sleeping
o
Have enough rest intervals
Medication History o
Over the counter medication (buscopan) before issio
VIII. Nursing Care Plans PROBLEM # 1: Decrease cardiac output related to altered heart rate/rhythm ASSESSMENT
S: ø
NURSING
SCIENTIFIC
DIAGNOSIS
EXPLANATION
Decrease cardiac output
Occlusion in the artery
O : The patient
related to altered
Decreased blood
manifested the
heart rate/rhythm
supply
following: Afebrile Conscious and coherent Pale palpebral
Decreased venous return Decreased
conjunctiva
amount of blood
With capillary refill
expelled by ventricles
time of 3 seconds
manifest: Decreased skin turgor Sunken eyeballs Sudden weight loss
Short term:
NURSING INTERVENTIONS 1.
Establish
RATIONALE
1.
EXPECTED OUTCOME
To gain
Short term:
After 1-2 hours of
therapeutic
trust of the
The patient
nursing
relationship
patient
shall have
interventions, the
To note any
participated in
patient will
patient’s
abnormaliti
activities that
participate in
general
es
reduce the
activities that reduce
condition
To have
workload of the
Take and
baseline
heart.
record the
data
the workload of the
2.
3.
heart.
Assess
patient’s vital . 4.
Decreasedcardiac output
The patient may
OBJECTIVES
5.
2.
3.
4.
For comfort
signs
and
Provide
hygiene to
morning care
the patient
Evaluate
5.
To assess
client reports
for signs of
and evidence
poor
of extreme
ventricular
fatigue,
function
intolerance of
and/or
activity and
impending
progressive
cardiac
shortness of
failure
Decreased urine output
breath 6.
Monitor
6.
To note
cardiac
effectivene
Vital signs
rhythm
ss of
taken:
continuously
medication
Decrease
s
T:36.9
7.
RR: 21
stimuli;
HR: 116
provide quiet
7.
adequate
environment
BP: 150/170 8.
9.
Schedule
To promote rest
8.
To
activities and
maximize
assessments
rest periods
Instruct client
9.
Which can
to avoid/limit
cause
activities
changes in
10. ncourage relaxation techniques 11. Provide for
cardiac pressures 10. To reduce anxiety and
diet
conserve
restrictions
energy
12. Encourage
11. To maintain
changing
adequate
positions
nutrition
slowly,
12. To reduce
dangling legs
risk for
before
orthostatic
standing
hypotensio
13. Give information
n 13. To provide
about
encourage
positive signs
ment
of improvement
PROBLEM # 2: Ineffective Peripheral Tissue Perfusion related to decreased cardiac output ASSESSMENT
NURSING
SCIENTIFIC
DIAGNOSIS
EXPLANATION
OBJECTIVES
NURSING INTERVENTIONS
RATIONALE
EXPECTED OUTCOME
S: ø
Ineffective
Ineffective tissue
Short term:
1.
Establish
1.
To build a
Short term:
Peripheral Tissue perfusion is the decrease
After 1-2 hours
therapeutic
good and
O : The patient
Perfusion related
in oxygen resulting in
of nursing
relationship
trusting
shall have
manifested the
to decreased
failure to nourish tissues
interventions,
Assess patient’s
relationship
verbalized
following:
cardiac output
at the capillary level. An
the patient will
general condition
with the
understanding
abrupt increase in
verbalize
Take and record the
patient
of condition,
pressure brings about a
understanding
patient’s vital signs
To assess for
therapy
Vital signs
rapid and reversible
of condition,
that contributes to
complications
regimen, side
taken:
vasoconstriction of small
therapy
the patient’s
To note and
effects of
T:36.9
resistance vessels due to
regimen, side
complaint.
assess for
medications,
RR: 21
their inherent myogenic
effects of
Note current
complicatons
and when to
HR: 116
tone. Prolonged
medications,
situation or
Affecting
BP: 150/170
elevations of pressure
and when to
presence of
systemic
healthcare
can cause a range of
conditions that can
circulation or
provider.
The patient may
more lasting changes in
healthcare
affect perfusion to
perfussion
manifest:
the microcirculation, 2 of
provider.
Hypertension
2.
3.
all body systems
3.
4.
Client at
olyguria
which, remodeling of
capillary refill
small arteries and
conditions
venous
arterioles and rarefaction
associated with
stasis, vessel
of arterioles and
thrombus or emboli
wall injury
Note location of
and
restrictive clothing,
hypercoagula
pressure dressings,
bility
time more than 3 seconds warm extremities
capillaries, will be
4.
2.
5.
considered briefly below.
cyanosis and
edema
higher risk for
circular wraps, cast,
pallor on extremities
Determine history of
6.
5.
That may
or traction device
restrict
Compare skin
circulation to
temperature and
limb. Helps
The patient
paresthesia
7.
color with other limb
differentiate
when assessing
type of
extremity circulation
problems
Assess presence,
6.
location, and degree
identifying or
of swelling or
quantifying
edema formation.
edema in
Measure capillary
involved
time 8.
9. 10. 11. 12.
13. 14.
Useful in
Note client’s
extremity 7.
To determine
nutritional and fluid
adequacy of
status
systemic
Inspect lower extremities for skin texture Palpate arterial pulses Determine pulse equality, as well as intensity Determine time that symptoms are worse, precipitating, or aggravating events Assess motor and sensory function ister medications such as antiplatelet agents, thrombolytics, antibiotics.
circulation 8.
Protein energy malnutrition and weight loss make ischemic tissues more prone to breakdown
9.
That often accompany diminished peripheral perfusion
10. To determine
level of circulatory blockage 11. To evaluate distribution and quality of blood flow, and success or failure of therapy 12. To help isolate and differentiate problems 13. Problems with ambulation; hypersensitivi ty or loss of sensation and numbness and tingling are changes that can indicate neurovascula r dysfunction
14. To improve tissue perfusion or organ function
PROBLEM # 3: Acute Pain as evidence by abdominal pain in the epigastric area secondary to intestinal obstruction
NURSING
SCIENTIFIC
S>O
DIAGNOSIS Acute Pain as
EXPLANATION Intestinal obstruction
O>patient
evidence
refers to a lack of
After 1-2 hours
condition.
manifested:
abdominal
movement
of
of
Monitor
>pain scale of
pain
intestinal
contents
7/10
epigastric area
through the intestine.
patientt will be
>bloatedness
secondary
Because
able to report
> + epigastric
intestinal
smaller
pain
obstruction
obstructions
ASSESSMENT
after
in
by the to
the
of
its
lumen, are
OBJECTIVES Short term:
interventions,
pain
in
epigastric
Vital signs
occur more rapidly in
area.
taken:
the small intestine,
T:36.9
but they can occur in
RR: 21
the large intestine as
BP: 150/170
the
cause
location,
Assess
2.
the
3.
4.
made
of
about
3.
interventio n is more
as soon as it
likely to be
begins
successful
provide comfort
in alleviating
position
-flank pain
example, twisting of
-distraction/
the
guarding
cause sudden total
behaviors
obstruction, whereas
-increased
a
provide
such
pain
of
4.
non-
quiet,
relaxing
pharmacol
environment
ogical pain
6.
5.
encourage
which
-diaphoresis
and discomfort.
activities
-sleep disturbance
7.
to provide adequate
diversional
could lead to pain
to provide
mgmt.
progressive
-pallor
timely
pt to report pain
situation.
obstruction
the
pain. Instruct the
-weakness
elevated BP
be
choices
change
or
info
encourage
gradually developing
PR,RR,
exact
treatment
manifest:
to
shall reported
pain
measures
leads
data
in
acute problem or a
could
the
can
of
rest
like
socialization with
periods
others and slow,
and
rhythmic
prevent
breathing
fatigue
6.
ister analgesics ordered
as
OUTCOME Short term:
baseline
assessment
may
5.
gather
significant
may manifest as an
tumor
a
To
comprehensive
The patient
For
2.
perform
feelings
and
1.
and
verbalization
obstruction
intestine
pt’s
record pt’s VS
decreased
more common and
well. Depending on
1.
EXPECTED
RATIONALE
INTERVENTIONS
nursing
eating
HR: 116
NURSING
to
these could draw the
pt’s
attention away from the pain
patient
decreased flank pain
in
PROBLEM #4: Activity intolerance r/t pain ASSESSMENT s> Ø
NURSING DIAGNOSIS Activity intolerance r/t
o> the patient
EXPLANATION Pain is an unpleasant sensory and emotional
Short term: After 2 hours
NURSING INTERVENTIONS 1. Establish rapport 2. Monitor VS 3. Note patient’s response
of NI, the patient
primarily associated
will identify
with tissue damage or
negative factors
describe in such
affecting activity
as damage, or both
intolerance and
Vital signs taken:
that can be a stressor
eliminate or
and move about and
T:36.9
in performing activities
reduce their
degree of assistance
Pain scale of 7/10 Complaints of pain
RR: 21
of daily living due to
HR: 116
the pain being
BP: 150/170
experienced with certain movements.
The patient may manifest:
OBJECTIVES
experience which I
manifested:
pain
SCIENTIFIC
May acquire risks related with
immobility Further difficulty with
mobility May develop insomnia due to severe pain
effects when possible.
of weakness, fatigue, pain, difficulty accomplishing tasks and/or insomnia 4. Ascertain ability to stand
necessary/use of equipment 5. Provide comfort measures and provide for relief for pain 6. Encourage patient to maintain positive attitude. 7. Instruct patient/SO (s) in monitoring response to activity 8. Plan for progressive increase of activity level, as tolerated by the patient 9. Involve patient/SO (s) in planning of activities
RATIONALE 1. To gain patient and trust and cooperation 2. To obtain baseline data 3. Symptoms may be result of/or contribute to activity intolerance 4. To determine current status and needs associated with participation in needed/desired activities 5. Enhance ability to participate in activities 6. To enhance sense of well being 7. To indicate need to alter activity level 8. Both activity tolerance and health status may improve with progressive
EXPECTED OUTCOME Short term: The patient shall have identified negative factors affecting activity intolerance and eliminate or reduce their effects when possible
PROBLEM #5: Readiness for enhanced knowledge as evidence by expressing interest in learning about disease condition ASSESSMENT
NURSING
SCIENTIFIC
DIAGNOSIS
EXPLANATION
OBJECTIVES
NURSING INTERVENTIONS 1.
S: ø
Establish
RATIONALE 1.
EXPECTED OUTCOME
To build a
Readiness for
The first requirement in
Short term:
therapeutic
good and
Short term:
enhanced
for wellness is a desire
After 1 hour of
relationship
trusting
The patient
O : The patient
knowledge as
to attain a higher level
nursing
Assess patient’s
relationship
shall have
manifested the
evidence by
of well being. The
interventions, the
general condition
with the
verbalized
following:
expressing
patient must express
patient will
patient
understanding
interest in
readiness to engage
verbalize
the patient’s vital
To assess
of information
to health
learning about
and learn interventions
understanding of
signs
for
gained.
teachings
disease
that will help him reach
information
client’s
complicatio
given
condition
that next level.
gained.
level of
ns
Listens intently
2. 3.
4.
Take and record 2.
Assessing a patient’s
knowledge about
knowledge
readiness to respond to
specific topic
assess for
of the topic
wellness diagnosis
Assist client to
complicatio
Explains
5.
involves patient
identify learning
The patient
interviews and
goals
may manifest:
interaction. And
Anxiety Restlessness Fear
To note and
ns 4.
Provides
Ascertain
opportunity
readiness for enhanced
preferred
to ensure
management describes
methods of
accuracy
a patient who is willing
learning
and
Assist client to
completene
in her own treatment by
identify ways to
ss of
following
integrate and use
knowledge
recommendations and
information in all
base for
helping set new goals
appropriate areas
future
and able to participate
6.
3.
7.
for herself.
learning 5.
Helps to frame or focus content to be learned
6.
Identifies best approach to facilitate learning
7.
Ability to apply or use information increases desire to learn and retain information
IX. Drug Study Medical Management IVF’s, BT, NGT feeding, Nebulization, TPN, Oxygen therapy, etc. a. IVF MEDICAL
DATE ORDERED,
MANAGEMENT/
DATE PERFORMED,
TREATMENT
DATE CHANGE
GENERAL
INDICATION OR
DESCRIPTION
PURPOSES
D5LR 1L X 8 HRS
Date ordered: July 2, 2015
For daily maintenance of body fluids and nutrition, and for rehydration.
Treatment for persons needing extra calories who
Date of Results:
cannot tolerate
July 2, 2015
fluid overload.
CLIENT’S RESPONSE TO TREATMENT The patient willingly accepted treatment and is kept hydrated as evidenced by continuous infusion,
Treatment of
improvement in his
shock.
condition and good skin turgor. There were no negative effects noted.
NURSING RESPONSIBILITIES: BEFORE THE PROCEDURE: 1. Assess vital signs for baseline data, skin turgor, bleeding tendencies, disease or 2. 3. 4. 5. 6. 7.
injury to extremities, status of veins to determine appropriate puncture site. Consider: How long the patient is likely to have IV What kinds of fluids will be infused What medications the patient will be receiving or is likely to receive Prepare equipment needed Perform hand hygiene
DURING THE PROCEDURE: 1. Prepare the client: Introduce self and client’s activity 2. Explain the procedure to the client (IV infusion can cause discomfort for a few seconds, but no discomfort while the solution is flowing) 3. Make sure that the client’s clothing or gown can be removed over IV apparatus, if necessary 4. Clean the skin site of entry 5. Assess IV site for any redness, swelling, tenderness, or drainage 6. Ensure appropriate IV flow AFTER THE PROCEDURE: 1. Label the IV with date and time of attachment 2. Document the time of the start of infusion, flow rate, amount and type of solution and client’s general response 3. Teach the client ways to maintain the infusion system 4. Instruct the client to inform any side effects 5. Monitor patient frequently for: 6. 7. 8. 9.
Signs of infiltration/sluggish flow signs of phlebitis/infection well time of catheter and need to be replaced Condition of catheter dressing
10. Check the level of the IVF:
Correct solution, medication, and volume. Check and regulate the drop rate. Change the IVF solution if needed. Do not connect flexible plastic.
b. Drugs
NAME OF
DATE
ROUTE OR
DRUGS,
ORDERED,
ISTRATION
GENERIC
DATE
DOSAGE AND
NAME, BRAND
TAKEN/GIVEN,
FREQUENCY OF
NAME
DATE CHANGED
ISTRATION
GENERAL
CLIENT’S
ACTION,
INDICATION OR
RESPONSE TO
MECHANISM OF
PURPOSES
THE
ACTION
MEDICATION
General action: Generic name:
Date ordered:
OMEPRAZOLE
July 2, 2015
Brand names: LOSEC
Date of Results: July 2, 2015
Antiulcer
It is use to
The patient did
decrease the
not experience
Mechanism of
amount of acid
any adverse
Action:
produced in the
effect.
40 mg TIV O.D.
Inhibits proton pump
PRILOSEC
activity by binding to hydrogenpotassium adenosine triphosphatase, located at secretory surface of gastric parietal cells, to suppress gastric acid secretion. Nursing Responsibilities BEFORE 1. Observe 10 R’s of istration of drugs 2. Check doctor’s order three times and the patient 3. Check the label of the drug, its name and its expiration date 4. Wash hands before handling the medication
stomach
5. Assess patient’s vital signs prior to istering the medication DURING 1. ister as indicated (right drug, right dosage, right frequency) 2. Clean the IV insertion for medication with a cotton ball with alcohol. 3. Gradually inject the drug into the port. Slow IV push to prevent infiltration and phlebitis. 4. ister cautiously and slowly with aseptic technique. AFTER 1. Observe for the sensitivity and side effects to the drug 2. Reassess patient’s level of pain at least 15 and 30 minutes after parenteral istration 3. Monitor circulatory and respiratory status and bladder and bowel function. 4. Caution ambulatory patient about getting out of bed or walking.
NAME OF
DATE ORDERED,
DRUGS,
DATE
GENERIC NAME,
TAKEN/GIVEN,
BRAND NAME
DATE CHANGED
ROUTE OR ISTRATION DOSAGE AND FREQUENCY OF ISTRATION
GENERAL ACTION, MECHANISM OF ACTION
INDICATION OR PURPOSES
Generic name:
Date ordered:
CEFUROXIME
July 2, 2015
Brand names:
Serious lower
Antibiotic
respiratory tract infection, UTI,
Mechanism of
skin or skin-
Action:
structure
CEFTIN,
Inhibits cell-wall
infections, bone
ZINACEF
synthesis,
of t
promoting osmotic
infection,
instability; usually
septicema,
bactericidal.
meningitis and
KEFUROX,
Date of Results:
750 g TIV Q8
General action:
July 2, 2015
gonorrhea - Pharyngitis and tonsillitis - Early lyme disease
Nursing Responsibilities BEFORE 6. Observe 10 R’s of istration of drugs 7. Check doctor’s order three times and the patient 8. Check the label of the drug, its name and its expiration date 9. Wash hands before handling the medication 10. Assess patient’s vital signs prior to istering the medication DURING 5. ister as indicated (right drug, right dosage, right frequency) 6. Clean the IV insertion for medication with a cotton ball with alcohol. 7. Gradually inject the drug into the port. Slow IV push to prevent infiltration and phlebitis. 8. ister cautiously and slowly with aseptic technique. AFTER 5. Observe for the sensitivity and side effects to the drug 6. Reassess patient’s level of pain at least 15 and 30 minutes after parenteral istration 7. Monitor circulatory and respiratory status and bladder and bowel function. 8. Caution ambulatory patient about getting out of bed or walking.
NAME OF DRUGS, GENERIC NAME, BRAND NAME
DATE ORDERED, DATE TAKEN/GIVEN, DATE CHANGED
ROUTE OR ISTRATION DOSAGE AND FREQUENCY OF ISTRATION
GENERAL ACTION, MECHANISM OF ACTION
INDICATION
OR PURPOSE
Generic name: METRONIDAZOLE
Date ordered: July 2, 2015
500 mg TIV Q8
General action:
- Amebic Liver
Antiprotozoal
abscess - Intestinal
Brand names: FLAGYL, FLAGYL
Date of Results: July 2, 2015
Mechanism of
amebiasis
action:
- Trichomonias
ER, FLORAZOLE
Direct acting
ER, NOVO-
trichomonicide and
NIDAZOLE,
amebicide that
FLAGYL IV RTU
works inside and outside the intestines. It's thought to enter the cells of microorganisms that contain nitroreductase. forming unstable compounds that binds to DNA and inhibit synthesis, causing cell death.
Nursing Responsibilities BEFORE 11. Observe 10 R’s of istration of drugs 12. Check doctor’s order three times and the patient 13. Check the label of the drug, its name and its expiration date 14. Wash hands before handling the medication 15. Assess patient’s vital signs prior to istering the medication DURING 9. ister as indicated (right drug, right dosage, right frequency) 10. Clean the IV insertion for medication with a cotton ball with alcohol. 11. Gradually inject the drug into the port. Slow IV push to prevent infiltration and phlebitis. 12. ister cautiously and slowly with aseptic technique. AFTER 9. Observe for the sensitivity and side effects to the drug 10. Reassess patient’s level of pain at least 15 and 30 minutes after parenteral istration 11. Monitor circulatory and respiratory status and bladder and bowel function. 12. Caution ambulatory patient about getting out of bed or walking.
c. Diet TYPE OF DIET
DATE ORDERED,
GENERAL
INDICATION
DATE
DESCRIPTION
SPECIFIC FOOD
CLIENT'S
TAKEN
RESPONSE AND
TAKEN/GIVEN,
REACTION TO
DATE CHANGED
THE DIET NPO
NPO (Nothing per
Date ordered:
Orem)
July 2, 2015
stands
for
Nothing Per Orem
take food or drink
which
through mouth.
means
nothing by mouth. Date of Results: July 2, 2015
Patient cannot
Doctors use this on
orders
when
they do not want the patient to take in any type of food or liquid by mouth. For instance, when a patient is getting ready
for
a
surgery, they are ordered for NPO.
None
Patient cannot eat by mouth thought he can still receive nutrients needed by his body via NGT
Nursing Responsibilities (NPO): Before: Check for the doctor’s order for type of diet preferred. Explain the importance and purpose of the prescribed diet. Place an NPO sign on the bed. Remove all foods at bedside and emphasize strict compliance on the diet regimen. During: Monitor patient closely for compliance of the diet. Reiterate diet frequently to the patient or SO. Check bedside for presence of food, remove if necessary. After: Assess patient’s condition. Document
TYPE OF DIET
NGT
DATE ORDERED,
GENERAL
DATE
DESCRIPTION
INDICATION
SPECIFIC FOOD
CLIENT'S
TAKEN
RESPONSE AND
TAKEN/GIVEN,
REACTION TO
DATE CHANGED
THE DIET
Date ordered: July 2, 2015 Date of Results: July 2, 2015
These are special It It is indicated to preparations for patients who are prevent further unable to digest increase in the solid foods. patient’s blood pressure and to lower down cholesterol levels.
none only
As stated by the
medications
patient, there's a feeling of discomfort.
IX. Health Teachings METHOD M: instructed the patient to take the following Omeprazole Cefuroxime Metronidazole E: Instructed the client to have adequate bed rest T: Instructed the client on strict compliance to medication and therapy H: Instructed patient to always have adequate rest periods in a comfortable position Instructed patient to avoid high fat and high sodium content food Instructed patient to schedule regular follow-up check-up appointments with physician to monitor progress O: Instructed client to continue therapy D: Instructed client on low fat low salt diet
Related Documents c2h70
Case Study Intestinal Obstruction 5h74x
November 2022 0
Intestinal Obstruction 285f68
April 2021 0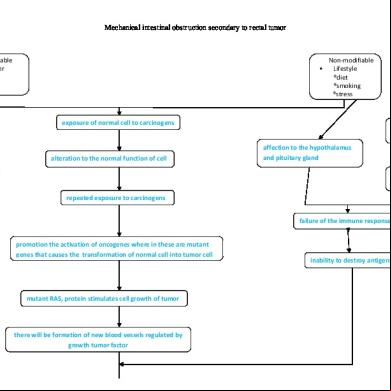
Pathophysiology Of Intestinal Obstruction 2c436e
October 2019 134
Case Study Intestinal Parasitism 5b2v2r
December 2019 54
Lecture Intestinal Obstruction (01)ppt d6m4r
December 2019 69
Nursing Diagnosis For Intestinal Obstruction 6w3j3q
October 2019 206More Documents from "Maria Paula Bungay" 6e444n
Case Study Intestinal Obstruction 5h74x
November 2022 0
6g3p1u
September 2022 0
Escuela Lombarda 1 2s5844
December 2022 0
6g3p1u
January 2023 0
Runt.doc 3ch36
December 2022 0