Carl Rogers _ Person-centered Theory.pdf 62h6u
This document was ed by and they confirmed that they have the permission to share it. If you are author or own the copyright of this book, please report to us by using this report form. Report 2z6p3t
Overview 5o1f4z
& View Carl Rogers _ Person-centered Theory.pdf as PDF for free.
More details 6z3438
- Words: 5,630
- Pages: 21
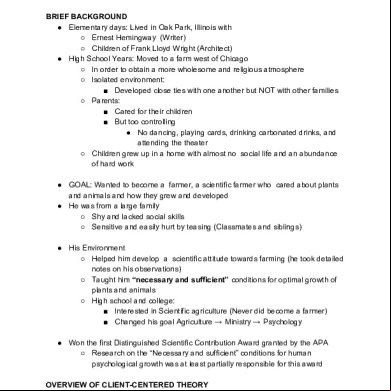
ROGERS: Person-Centered Theory BRIEF BACKGROUND ● Elementary days: Lived in Oak Park, Illinois with ○ Ernest Hemingway (Writer) ○ Children of Frank Lloyd Wright (Architect) ● High School Years: Moved to a farm west of Chicago ○ In order to obtain a more wholesome and religious atmosphere ○ Isolated environment: ■ Developed close ties with one another but NOT with other families ○ Parents: ■ Cared for their children ■ But too controlling ● No dancing, playing cards, drinking carbonated drinks, and attending the theater ○ Children grew up in a home with almost no social life and an abundance of hard work ● GOAL: Wanted to become a farmer, a scientific farmer who cared about plants and animals and how they grew and developed ● He was from a large family ○ Shy and lacked social skills ○ Sensitive and easily hurt by teasing (Classmates and siblings) ● His Environment ○ Helped him develop a scientific attitude towards farming (he took detailed notes on his observations) ○ Taught him “necessary and sufficient” conditions for optimal growth of plants and animals ○ High school and college: ■ Interested in Scientific agriculture (Never did become a farmer) ■ Changed his goal Agriculture → Ministry → Psychology ● Won the first Distinguished Scientific Contribution Award granted by the APA ○ Research on the “Necessary and sufficient” conditions for human psychological growth was at least partially responsible for this award OVERVIEW OF CLIENT-CENTERED THEORY ● Carl Rogers → Founder of Client-Centered Therapy
Rogers ● Consummate therapist ● Reluctant Theorist
Freud ● Theorist (Primarily) ● Therapist (Secondarily)
● More concerned with helping people than discovering why they behaved the way they did. ● Asks, “How can I help this person grow and develop?” rather than “What caused this person to develop this manner?” ● Called for Empirical Research in both his personality theory and therapeutic approach ● Advocated a balance between tender-minded and hardheaded studies that would expand knowledge of how humans feel and think ● Formulated an internally consistent theory of personality ○ Not comfortable with the notion of theory ○ Personal preference: Helper of people rather than a constructor of theories ■ Theories seemed too cold and external ● 1950’s → He was incited to write the “Client-Centered” Theory of personality ○ His original statement is found in Volume 3 of Sigmund Koch’s Psychology: A Study of a Science ● Rogers was aware that 10 or 20 years, his theories would be different ● Througout the intervening years ○ He did not systematically reformulated his theory of personality ○ His final theory of personality rests on that original foundation spelled out in Koch series BIOGRAPHY OF CARL ROGERS (KRISTINE) CARL RANSOM ROGERS ● born on January 8, 1902 in Oak Park, Ilinois ● Parents: Walter and Julia Cushing Rogers ● He intended to become a farmer but later on became more devoted to religion. ○ He traveled to China for 6 months to attend a student religious conference where the interaction with other young religious leaders changed him into a more liberal thinker and moved him toward independence from the religious views of his parents. ○ He returned from the journey with ulcer which prevented him from immediately going back to the university.
○ After a year, he returned to Wisconsin where he displayed more self-confidence and became a changed student from his pre-China days. 1924 - Rogers entered the Union Theological Seminary in New York to become a minister. ● He enrolled in several psychology and education courses at neighboring Columbia University. ● John Dewey - prominent at Teachers College, Columbia whose progressive education movement influenced Rogers ● Gradually, Rogers became disenchanted with the dotrinaire attitude of religious work and desired mored freedom to explore new ideas. ○ 1926 - He left the seminary to attend Teachers College in a full-time basis with a major in clinical and educational psychology. 1927 - Rogers worked at the new Institute for Child Guidance in New York City while completing his doctoral degree. He gained an elementary knowledge of Freudian psychoanalysis but he was not much influenced by it. 1931 - He received his PhD from Columbia. ● Otto Rank - one of Freud’s closest associates before his dismissal from Freud’s inner circle whose ideas strongly influenced Rogers. ● He was invited by Rogers for a 3-day seminar at Rochester to present his new post-Freudian practice of psychotherapy ○ Therapy is an emotional growth-producing relationship, nurtured by the therapist’s empathic listening a nd unconditional acceptance of the client. Rogers harbored a desire to teach in a university after a rewarding teaching experience during the summer of 1935. ● During this time, he published his first book, The Clinical Treatment of the Problem Child (1939) which led to a teaching offering from Ohio State University. ● His wife urged him to accept the offer and Ohio State agreed to hire him as a full professor. ● In 1940, at the age of 38, Rogers moved to Columbus to begin a new career. At Ohio State University, Rogers began to conceptualize his own ideas on psychotherapy. ● 1942 - He published Counseling and Psychotherapy, a reaction to the okder approaches to therapy that emphasized the importance of growth within the patient.
Rogers moved back to New York as director of counseling services for the United Services Organization then later on established a counseling center. ● His therapy improved from one that emphasized methodology (nondirective technique) t o one that emphasizes client-therapist relationship. 1957 - Rogers accepted a position at the University of Wisconsin but became frustrated because he was unable to unite the professions of psychiatry and psychology. ● He left his job at Wisconsin and moved to California where he ed the Western Behavioral Sciences Institute (WBSI) ● He resigned from WBSI when he felt it was becoming less democratic and formed the Center for Studies of the Person. February 4, 1987 - Rogers died following surgery for a broken hip. The personal life of Carl Rogers was marked by change and openness to experience. ● He was extremely shy as an adolescent but had an active fantasy life. ● Helen Elliott - the only young lady he had known in elementary school in Oak Park whom he had enough courage to ask out ● 1924 - Helen and Carl were married and had two children named David and Natalie. ● Despite his early problems with interpersonal relationships, Rogers grew to become a leading proponent of the notion that the interpersonal relationship between two individuals is a powerful ingredient that cultivates psychological growth within both persons. Honors received: ● First president of the American Association for Applied Psychology ● President of American Psychological Association (APA) for 1946-1947 ● First president of the American Academy of Psychotherapists ● Cowinner of the first Distinguished Scientific Contribution Award presented by APA in 1956
PERSON-CENTERED THEORY Basic Assumptions (ALLIEAH) Formative Tendency - tendency for all matter, both organic and inorganic, to evolve from simpler to more complex forms. Actualizing Tendency - tendency for all humans to move toward completion or fulfillment of potentials. - the only motive people possess.
-
eg. the need to satisfy hunger drive, express deep emotions and accept one's self Need for maintenance - includes basic needs as food, air and safety - also includes tendency to resist change and to seek the status quo
● ●
●
● ●
Enhancement - need to become more, to develop and to achieve growth - seen in people's willingness to learn things that are not immediately rewarding. enhancement needs - expressed through curiosity, playfulness, self exploration, friendship and confidence that one can achieve psychological growth. Actualization tendency is NOT limited to humans and is realized only under certain conditions. People must be involved in a relationship with a partner who is: ○ Congruent or authentic ○ Demonstrates empathy and ○ unconditional positive regard Rogers: These three qualities DOES NOT cause people to move toward constructive personal change but, permit them to actualize their innate tendency toward self-fulfillment. These conditions are both necessary and sufficient conditions for becoming self-actualized person. Only humans have a concept of self and thus, a potential for self-actualization.
The Self and Self-Actualization (BRENT) The Self-Concept ● Includes aspects of one’s beings and experiences that are perceived in awareness (not always accurate) by the individual. ○ NOT identical with the organic self. ○ Portions of organismic self may be beyond a person’s awareness or simply not owned by that person. ○ EXAMPLE: Stomach is part of the organismic self, but it is not likely to be a part of one’s self-concept unless it malfunctions and causes concern ● Once people form their self-concept, they find change and significant learning quite difficult.
○ Experiences that are inconsistent with their self-concept are either denied or accepted only in distorted forms. The Ideal Self ● One’s view of the self as one wishes to be ● Contains all those attributes that people aspire to possess. ● Wide gap between the ideal self and self-concept indicates incongruence and unhealthy personality. ● Psychologically healthy individuals perceive little discrepancy between their self-concept and what they ideally would like to be.
Awareness (AKI) ● Is the symbolic representation of some portion of our experience ● Without awareness self-concept and the ideal self would not exist Levels of Awareness ● 3 levels ○ 1st: there are experienced events that may be either ignored or denied ○ 2nd: some experiences are accurately symbolized and freely itted to the self-structure ○ 3rd: involved experiences that are perceived in a distorted form (we reshape or distort the experience for it to be consistent with our view of self) Denial of Positive Experiences ● Not only negative or derogatory experiences that are distorted or denied to awareness; many people also have difficulty in accepting positive and genuine compliments ● They may be distorted because the person distrusts the giver, or they may be denied because the recipient does not feel deserving of them ● A compliment from another also implies the right of that person to criticize or condemn, and thus the compliment carries an implied threat Becoming a Person (AKI) ● First, an individual must make (positive or negative) with another person ○ In order to survive, an infant must experience some from a parent or caregiver
● As children (or adults) become aware that another person has some measure of regard for them, they begin to value positive regard and devalue negative regard ○ That is, the person develops a need for positive regard (love, liked, or accepted by another person) ○ If we perceive that other/significant others value us, then our need for positive regard is at least partially satisfied ● Positive regard is a prerequisite for positive self-regard (defined as the experience of prizing or valuing one’s self) ● Once positive self-regard is established, it becomes independent of the continual need to be loved ● The source of positive self-regard, then, lies in the positive regard we receive from others ○ But once established, it is autonomous and self-perpetuating Barriers to Psychological Health - Not everyone becomes a healthy person. Most people experience the four barriers to psychological health. Conditions of Worth - People perceive that their parents, peers or partners love and accept them only if they meet those people’s expectations and approval. - Arises when the positive regard of a significant other is conditional, when the individual feels that in some respects he/she is prized and in others not - Criterion by which we accept or reject our experiences - If we see that others accept us regardless of our actions, then we come to believe that we are prized unconditionally. - If we perceive that some of our behaviors are approved and some disapproved, then we see that our worth is conditional. - We introject the values of others - External Evaluations: our perceptions of other people’s view of us - Prevent us from being completely open to our own experiences - Example: We may reject pleasurable experiences because we believe that other people do not approve of them Incongruence - Organism and the self are two separate entities (may or may not be congruent with one another)
-
Psychological disequilibrium : begins when we fail to recognize our organismic experiences as self-experiences Source of psychological disorders Conditions of Worth → Self-concept → Incongruence
A. Vulnerability - The greater the incongruence between our perceived self/self-concept and our organismic experience, the more valuable we are. - People are vulnerable when they are unaware of the discrepancy between their organismic self and their significant experience - Often behave in ways that are incomprehensible not only to others but also to themselves B. Anxiety and Threat - Anxiety: state of uneasiness or tension whose cause is unknown - When we become dimly aware that the discrepancy between our organismic experience and our self-concept may become conscious - As we become more aware of the incongruence between our organismic experience and our self-concept, our anxiety evolves into threat - Represent steps toward psychological health - These two signal to us that our organismic experience is inconsistent with our self-concept Defensiveness (ROSE) - In order to prevent the inconsistency between our organismic experience and our perceived self, we react in a defensive manner - Defensiveness - the protection of self-concept against anxiety and threat by the denial or distortion of experiences inconsistent with it - When our experiences is inconsistent with one part of our self-concept, we will behave in a defensive manner in order to protect the current structure of our self-concept - 2 chief defenses: distortion and denial - Distortion - We misinterpret an experience in order to fit it into some aspect of our self-concept
-
-
-
-
-
-
We perceive the experience in awareness, but we fail to understand its true meaning - Denial - We refuse to perceive an experience in awareness, or at least we keep some aspect of it from reaching symbolization - Not as common as distortion because most experiences can be twisted or reshaped to fit the current self-concept ● Distortion and denial serve the same purpose: they keep our perception of our organismic experiences consistent with our self-concept which allows us to block out experiences that otherwise would cause unpleasant anxiety or threat Disorganization (ROSE) Most people engage in defensive behavior, but sometimes defenses fail and behavior becomes disorganized or psychotic We must trace the course of disorganized behavior, which has the same origins as normal defensive behavior, namely a discrepancy between people’s organismic experience and their view of self. Denial and distortion are adequate to keep normal people from recognizing this discrepancy, but when the incongruence between people’s perceived self and their organismic experience is either too obvious or occurs too suddenly to be denied or distorted, their behavior becomes disorganized. Disorganization can occur suddenly, or it can take place gradually over a long period of time. In a state of disorganization, people sometimes behave consistently with their organismic experience and sometimes in accordance with their shattered self-concept - Example 1:First case is a previously prudish and proper woman who suddenly begins to use language explicitly sexual and scatological - Example 2: The second case can be illustrated by a man who, because his self-concept is no longer a gestalt or unied whole, begins to behave in a confused, inconsistent, and totally unpredictable manner. In both cases, behavior is still consistent with the self-concept, but the self-concept has been broken and thus the behavior appears bizarre and confusing. Rogers always remained uncomfortable with the “neurotic” and “psychotic,” preferring instead to speak of “defensive” and “disorganized” behaviors, that more accurately convey the idea that psychological maladjustment is on a continuum from the slightest discrepancy between self and experience to the most incongruent
PSYCHOTHERAPY Conditions (ELAINE) In order for therapeutic growth to take place, the following conditions are necessary and sufficient: 1. Anxious or vulnerable client must come into with a congruent therapist who also possesses empathy and unconditional positive regard for that client. 2. The client must perceive these characteristics in the therapist. 3. There must be some duration for the between client and therapist Note: The first and third conditions are present with nearly any psychotherapy ● Client-centered therapy: unique in its insistence that the conditions of counselor congruence, unconditional positive regard, and empathic listening are both necessary and sufficient. - Congruence: general quality possessed by the therapist - Unconditional positive regard & emphatic listening: specific feelings or attitudes that the therapist has for an individual client Counselor Congruence ( ELAINE) - Congruence: exists when a person’s organismic experiences are matched by an awareness of them and by ability and willingness to openly express these feelings - To be real or genuine - To be whole or integrated - To be what one truly is - Congruent therapist: First necessary and sufficient condition for therapeutic change - Congruent counselor: a complete human being with feelings of joy, anger, frustration, confusion - Despite being constantly exposed to new organismic experiences, they accept these experiences into awareness -> psychological growth - They wear no mask, do not attempt to fake a pleasant facade,and avoid any pretense of friendliness and affection when these emotions are no truly felt - They are able to match feelings with awareness and both with honest expression - Congruence involves: feelings, awareness, expression
-
Incongruence can arise from either of the two points dividing these three experiences. 1. Breakdown between feelings and awareness: a person may be feeling angry, and the anger may be obvious to others; but the angry person is unaware of the feeling. 2. Discrepancy between awareness of an experience and the ability or willingness to express it to another: “I know I’m feeling bored by what is being said, but I don’t dare verbalize my disinterest because my client will think that I am not a good therapist” ● Rogers: therapists will be more effective if they communicate genuine feelings, even when those feelings are negative or threatening ● To do otherwise would be dishonest, clients will detect any significant indicators of incongruence. ● Rogers: Although congruence is a necessary ingredient in successful therapy, it is not necessary for a therapist to be congruent in all relationships outside the therapeutic process. ○ One can be less than perfect yet an effective psychotherapist ○ One need not be absolutely congruent in order to facilitate some growth within a client ○ Different degrees of congruence exist with unconditional positive regard and empathic listening. ● THE MORE THE CLIENT PERCEIVES EACH OF THESE QUALITIES AS CHARACTERIZING THE THERAPIST, THE MORE SUCCESSFUL WILL BE THE THERAPEUTIC PROCESS. Unconditional Positive Regard ( KATHLEEN) ● Unconditional - positive regard is no longer dependent on specific client behaviors and does not have to be continually earned. ● Positive - indicates that the direction of the relationship is toward warm and caring feelings ● Regard - there is a close relationship and that the therapist sees the client as an important person ● Positive regard - the need to be liked, prized, or accepted by another person. ● Unconditional positive regard - need that exists without any conditions or qualifications
○ “experiencing a warm, positive and accepting attitude toward what is the client” ○ without possessiveness, without evaluations, and without reservations ○ shows a nonpossessive warmth and acceptance, not an effusive, effervescent persona. ■ caring for others without smothering or owning that person. ■ allowing others you care to be autonomous and independent of your evaluations and restrictions. ■ respecting that others have their own feelings and opinions ■ letting the other person be its own self by making it decide for itself ■ in short, mind your own business at may sarili siyang kakayahan sa buhay nya :3 ● Therapists: ■ Must be client-centered and actively involved in a relationship with the client. ■ they must accept and prize their clients without any restrictions or reservations and without regard to the clients’ behavior. ■ may value some client behaviors more than others ■ positive regard must remain constant and unwavering. ■ Must not evaluate clients, nor do they accept one action and reject another. ● External evaluation leads to clients’ defensiveness and prevents psychological growth.
Empathic Listening (KATHLEEN) ● Necessary and sufficient of psychological growth ● Empathy - exists when therapists accurately sense the feelings of their clients and are able to communicate these perceptions - Being able to enter the world of feelings without prejudice, projection, or evaluation. - Roger: “means temporarily living in the other’s life, moving about in it delicately without making judgments” - does not involve interpreting clients’ meanings or uncovering their unconscious feelings, procedures that would entail an external frame of reference and a threat to clients. - suggests that a therapist sees things from the client’s point of view and that the client feels safe and unthreatened.
-
effective because it enables clients to listen to themselves and, in effect, become their own therapists.
EMPATHY
SYMPATHY
A feeling with a client
A feeling for a client Never therapeutic Stems from external evaluation Leads to client’s self-pity - Threatens positive self-concept - Creates self-structure disequilibrium
● Empathic listening - a powerful tool that facilitates personal growth within the client. ● Empathy in effect - When persons are perceptively understood, they find themselves coming in closer touch with a wider range of their experiencing. - Find people which they can turn for guidance in understanding themselves and directing their behavior. - If accurate and deep, they may also be able to unblock a flow of experiencing and permit it to run its uninhibited course. ● An empathic therapist ○ do not take empathy for granted ○ checks the accuracy of their sensings by trying them out on the client. ○ does not have the same feelings as the client ○ does not feel anger, frustration, confusion, resentment, or sexual attraction at the same time a client experiences them. ○ experiences the depth of the client’s feeling while permitting the client to be a separate person. ○ has an emotional as well as a cognitive reaction to a client’s feelings not belonging to the therapist, but the feelings belong to the client ○ does not take ownership of a client’s experiences ○ able to convey to the client an understanding of what it means to be the client at that particular moment Process If the conditions of therapist congruence, unconditional positive regard, and empathy are present, then the process of therapeutic change will be set in motion.
Stages of Therapeutic Change
The process of constructive personality change can be placed on a continuum from most
defensive to most integrated. Rogers (1961) arbitrarily divided this continuum into seven stages. Stage 1
● ●
characterized by an unwillingness to communicate anything about oneself. People at this stage ordinarily do not seek help, but if for some reason they come to therapy, they are extremely rigid and resistant to change.
Stage 2
● ●
clients become slightly less rigid. They discuss external events and other people, but they still disown or fail to recognize their own feelings. (feelings were such objective phenomena).
Stage 3
● ●
more freely talk about self, although still as an object. Clients talk about feelings and emotions in the past or future tense and avoid present feelings. vaguely perceive that they can make personal choices, and deny individual responsibility for most of their decisions
● Stage 4
● ● ●
●
Stage 5
● ● ●
● Stage 6
● ● ● ● ●
begin to talk of deep feelings but not ones presently felt. They deny or distort experiences, although they may have some dim recognition that they are capable of feeling emotions in the present. They begin to question some values that have been introjected from others, and they start to see the incongruence between their perceived self and their organismic experience. They accept more freedom and responsibility than they did in Stage 3 and begin to tentatively allow themselves to become involved in a relationship with the therapist. they have begun to undergo significant change and growth. They can express feelings in the present, although they have not yet accurately symbolized those feelings. They are beginning to rely on an internal locus of evaluation for their feelings and to make fresh and new discoveries about themselves. They also experience a greater differentiation of feelings and develop more appreciation for nuances among them. In addition, they begin to make their own decisions and to accept responsibility for their choices experience dramatic growth and an irreversible movement toward becoming fully functioning or self-actualizing. They freely allow into awareness those experiences that they had previously denied or distorted. They become more congruent and are able to match their present experiences with awareness and with open expression. They no longer evaluate their own behavior from an external viewpoint but rely on their organismic self as the criterion for evaluating experiences. They begin to develop unconditional self-regard, which means that they have a feeling of genuine caring and affection for the person they are
●
Stage 7
● ● ● ●
●
becoming. An interesting concomitant to this stage is a physiological loosening. These people experience their whole organismic self, as their muscles relax, tears flow, circulation improves, and physical symptoms disappear. occur outside the therapeutic encounter, because growth at Stage 6 seems to be irreversible. “persons of tomorrow” They are able to generalize their in-therapy experiences to their world beyond therapy. They possess the confidence to be themselves at all times, to own and to feel deeply the totality of their experiences, and to live those experiences in the present. People receive pleasure in knowing that these evaluations are fluid and that change and growth will continue. In addition, they become congruent, possess unconditional positive self-regard, and are able to be loving and empathic toward others.
Theoretical Explanation for Change When people come to experience themselves as prized and unconditionally accepted, they realize, perhaps for the first time, that they are lovable. ● As clients perceive that they are emphatically understood, they are freed to listen to themselves more accurately, to have empathy for their own feelings. ● As a consequence, when these persons come to prize themselves and to accurately understand themselves, their perceived self becomes more congruent with their organismic experiences. ● They now possess the same three therapeutic characteristics as any effective helper, and in effect, they become their own therapist. Outcomes (MARION) ● The most basic outcome of successful client-centered therapy is a congruent client ○ less defensive and more open to experience ○ have a clearer picture of themselves and a more realistic view of the world ○ Can assimilate experiences into the self on the symbolic level ○ they are more effective in solving problems ○ they have a higher level of positive self-regard. ● More realistic ○ Accurate view of potentials which narrows the gap between ideal and actual self ● less physiological and psychological tension
● ● ● ●
More accepting of others more mature, likeable, and socialized Their genuineness, positive self-regard and empathic ununderstanding are extended beyond therapy, and they become better able to participate in other growth-facilitating relationships
THE PERSON OF TOMORROW - If the three necessary and sufficient therapeutic conditions are optimal, a person of tomorrow will emerge. - Person of tomorrow = fully functioning people; psychologically healthy individuals - There are eight characteristics of a person of tomorrow: (1) MORE ADAPTABLE ❏ More likely to survive from an evolutionary perspective ❏ Realization that conformity and adjustment to a fixed condition have little long-term survival value (2) OPEN TO THEIR EXPERIENCES
❏ Do not deny or distort experiences ❏ All internal and external stimuli are freely received by the self ❏ Listen to themselves and hear their emotions e.g. joy, anger, fear (3) TRUST IN THEIR ORGANISMIC SELVES ❏ ❏ ❏ ❏
Do not depend on others for guidance Use own experiences as best criteria when making choices Trust their own inner feelings when making decisions Take into consideration the rights and feelings of others which they see clearly when making decisions
(4) LIVE FULLY IN THE MOMENT ❏ See each experience with a new freshness and appreciate it fully in the present ❏ Existential tendency: the tendency to live in the moment ❏ No need to deceive themselves and no reason to impress others ❏ No preconceptions about how the world should be ❏ Live the experience without prejudice of prior expectations (5) EXPERIENCE HARMONIOUS RELATIONS WITH OTHERS ❏ ❏ ❏ ❏
Feel no need to be liked or loved by everyone Know that they are unconditionally prized and accepted by someone Authentic in their relations with others Show care towards others without prejudice
(6) MORE INTEGRATED ❏ ❏ ❏ ❏ ❏
More whole individual See differences clearly Bridge the gap between real self and ideal self Present no facades to other people Openly express whatever feelings they are experiencing
(7) HAS BASIC TRUST OF HUMAN NATURE ❏ Would not harm others for personal gain ❏ Would care about others and ready to offer help when needed ❏ Do not strike out unreasonably against others
❏ Channel aggression in appropriate directions (8) ENJOY A GREATER RICHNESS OF LIFE ❏ Feel more deeply than others ❏ Live in the present and participate in the moment more fully than others PHILOSOPHY OF SCIENCE (JORDAN) ●
Science begins and ends with the subjective experience, everything in between must be objective and empirical.
What a scientist should be ●
● ●
Scientists must have characteristics of the person of tomorrow ○ look within ○ be in tune with internal feelings and values ○ be intuitive and creative ○ be open to experiences ○ welcome change ○ have a fresh outlook ○ possess a solid trust in themselves scientists should care for newly born ideas and nurture them lovingly scientists should be completely involved in the phenomena being studied ○ ex. People who conduct research on psychotherapy must first have had long careers as therapists.
How Science Happens ●
●
●
An intuitive scientist perceives patterns among phenomena. (may be too vague to communicate, but are nourished by a scientist to become a testable hypothesis) ○ hypothesis comes from an open-minded scientist, not stereotypical thoughts Methodology - must be rigorously controlled, empirical, and objective ○ precise methods prevent self-deception and from intentionally or unintentionally manipulating the observations (only the method of science that is precise and objective, not science itself) Scientist communicates findings from that method to others, ○ communication itself is subjective: The people receiving the communication bring their own degrees of open-mindedness or defensiveness into this process.
THE CHICAGO STUDIES (ANDREA) ● Rogers did not permit methodology to dictate the nature of his research ○ Allowed the problem to take precedence over methodology and measurement ○ They began by sensing vague impressions from clinical experience and gradually forming these into testable hypotheses ● Purpose: investigate both the process and the outcomes of client-centered therapy Hypotheses (ANDREA) ● States that all persons have within themselves the capacity, either active or latent, for self-understanding as well as the capacity and tendency to move in the direction of self-actualization and maturity. ● During therapy, clients would assimilate into their self-concepts those feelings and experiences previously denied to awareness. ● During and after therapy, the discrepancy between real self and ideal self would diminish and behavior of clients would be more socialized, more self-accepting, and more accepting of others. Method (ANDREA) ● Difficulty in selecting measuring instruments ○ Because the hypothesis dictates that subtle subjective personality changes should be measured objectively ● Used Thematic Apperception Test (TAT) ○ Projective personality test developed by Henry Murray ○ Used to test hypothesis that called for a standard clinical diagnosis ● Used Self-Other Attitude Scale (S-O Scale) ○ Instrument compiled at the Counseling Center from several earlier sources ○ Measures antidemocratic trends and ethnocentrism ● Used Willoughby Emotional Maturity Scale (E-M Scale) ○ Used to compare descriptions of clients’ behavior and emotional maturity as seen by two close friends and the clients themselves ● Used Q sort technique ○ Developed by William Stephenson ○ Measures changes from the client’s point of view ○ Begins with a universe of 100 self-referent statements printed on 3x5 cards
○ Participants are requested to sort into nine piles from “most like me” to “least like me” ○ Resulting distribution approximates a normal curve and allows for stat analysis ○ Participants were also requested to sort the cards to describe their self, their ideal self, and the ordinary person ● Participants ○ 18 men and 11 women who had sought therapy at Counseling Center ○ Called the experimental or therapy group ○ Received at least 6 therapeutic interviews and each session was recorded and transcibed ■ A procedure Rogers pioneered ● Methods of Control First Control ○ Own-Control or Wait Group ■ Participants waited 60 days before they would receive therapy ■ In order to determine if motivation to change rather than the therapy itself might cause people to get better ○ No-Wait Group ■ Received therapy immediately Second Control ○ Consisted of a separate group of “normals” ■ This comparison group allowed researchers to determine the effects of such variables as age of time, knowledge that one is part of an experiment (placebo effect), and impact of repeated testing ■ Divided into wait group and no-wait group
● Both were tested 4 times ○ At the beginning of 60-day wait period ○ Prior to therapy ○ Immediately after therapy ○ After a 6-12-months follow-up period Findings (LEI) Summary of Results (LEI)
Rogers ● Consummate therapist ● Reluctant Theorist
Freud ● Theorist (Primarily) ● Therapist (Secondarily)
● More concerned with helping people than discovering why they behaved the way they did. ● Asks, “How can I help this person grow and develop?” rather than “What caused this person to develop this manner?” ● Called for Empirical Research in both his personality theory and therapeutic approach ● Advocated a balance between tender-minded and hardheaded studies that would expand knowledge of how humans feel and think ● Formulated an internally consistent theory of personality ○ Not comfortable with the notion of theory ○ Personal preference: Helper of people rather than a constructor of theories ■ Theories seemed too cold and external ● 1950’s → He was incited to write the “Client-Centered” Theory of personality ○ His original statement is found in Volume 3 of Sigmund Koch’s Psychology: A Study of a Science ● Rogers was aware that 10 or 20 years, his theories would be different ● Througout the intervening years ○ He did not systematically reformulated his theory of personality ○ His final theory of personality rests on that original foundation spelled out in Koch series BIOGRAPHY OF CARL ROGERS (KRISTINE) CARL RANSOM ROGERS ● born on January 8, 1902 in Oak Park, Ilinois ● Parents: Walter and Julia Cushing Rogers ● He intended to become a farmer but later on became more devoted to religion. ○ He traveled to China for 6 months to attend a student religious conference where the interaction with other young religious leaders changed him into a more liberal thinker and moved him toward independence from the religious views of his parents. ○ He returned from the journey with ulcer which prevented him from immediately going back to the university.
○ After a year, he returned to Wisconsin where he displayed more self-confidence and became a changed student from his pre-China days. 1924 - Rogers entered the Union Theological Seminary in New York to become a minister. ● He enrolled in several psychology and education courses at neighboring Columbia University. ● John Dewey - prominent at Teachers College, Columbia whose progressive education movement influenced Rogers ● Gradually, Rogers became disenchanted with the dotrinaire attitude of religious work and desired mored freedom to explore new ideas. ○ 1926 - He left the seminary to attend Teachers College in a full-time basis with a major in clinical and educational psychology. 1927 - Rogers worked at the new Institute for Child Guidance in New York City while completing his doctoral degree. He gained an elementary knowledge of Freudian psychoanalysis but he was not much influenced by it. 1931 - He received his PhD from Columbia. ● Otto Rank - one of Freud’s closest associates before his dismissal from Freud’s inner circle whose ideas strongly influenced Rogers. ● He was invited by Rogers for a 3-day seminar at Rochester to present his new post-Freudian practice of psychotherapy ○ Therapy is an emotional growth-producing relationship, nurtured by the therapist’s empathic listening a nd unconditional acceptance of the client. Rogers harbored a desire to teach in a university after a rewarding teaching experience during the summer of 1935. ● During this time, he published his first book, The Clinical Treatment of the Problem Child (1939) which led to a teaching offering from Ohio State University. ● His wife urged him to accept the offer and Ohio State agreed to hire him as a full professor. ● In 1940, at the age of 38, Rogers moved to Columbus to begin a new career. At Ohio State University, Rogers began to conceptualize his own ideas on psychotherapy. ● 1942 - He published Counseling and Psychotherapy, a reaction to the okder approaches to therapy that emphasized the importance of growth within the patient.
Rogers moved back to New York as director of counseling services for the United Services Organization then later on established a counseling center. ● His therapy improved from one that emphasized methodology (nondirective technique) t o one that emphasizes client-therapist relationship. 1957 - Rogers accepted a position at the University of Wisconsin but became frustrated because he was unable to unite the professions of psychiatry and psychology. ● He left his job at Wisconsin and moved to California where he ed the Western Behavioral Sciences Institute (WBSI) ● He resigned from WBSI when he felt it was becoming less democratic and formed the Center for Studies of the Person. February 4, 1987 - Rogers died following surgery for a broken hip. The personal life of Carl Rogers was marked by change and openness to experience. ● He was extremely shy as an adolescent but had an active fantasy life. ● Helen Elliott - the only young lady he had known in elementary school in Oak Park whom he had enough courage to ask out ● 1924 - Helen and Carl were married and had two children named David and Natalie. ● Despite his early problems with interpersonal relationships, Rogers grew to become a leading proponent of the notion that the interpersonal relationship between two individuals is a powerful ingredient that cultivates psychological growth within both persons. Honors received: ● First president of the American Association for Applied Psychology ● President of American Psychological Association (APA) for 1946-1947 ● First president of the American Academy of Psychotherapists ● Cowinner of the first Distinguished Scientific Contribution Award presented by APA in 1956
PERSON-CENTERED THEORY Basic Assumptions (ALLIEAH) Formative Tendency - tendency for all matter, both organic and inorganic, to evolve from simpler to more complex forms. Actualizing Tendency - tendency for all humans to move toward completion or fulfillment of potentials. - the only motive people possess.
-
eg. the need to satisfy hunger drive, express deep emotions and accept one's self Need for maintenance - includes basic needs as food, air and safety - also includes tendency to resist change and to seek the status quo
● ●
●
● ●
Enhancement - need to become more, to develop and to achieve growth - seen in people's willingness to learn things that are not immediately rewarding. enhancement needs - expressed through curiosity, playfulness, self exploration, friendship and confidence that one can achieve psychological growth. Actualization tendency is NOT limited to humans and is realized only under certain conditions. People must be involved in a relationship with a partner who is: ○ Congruent or authentic ○ Demonstrates empathy and ○ unconditional positive regard Rogers: These three qualities DOES NOT cause people to move toward constructive personal change but, permit them to actualize their innate tendency toward self-fulfillment. These conditions are both necessary and sufficient conditions for becoming self-actualized person. Only humans have a concept of self and thus, a potential for self-actualization.
The Self and Self-Actualization (BRENT) The Self-Concept ● Includes aspects of one’s beings and experiences that are perceived in awareness (not always accurate) by the individual. ○ NOT identical with the organic self. ○ Portions of organismic self may be beyond a person’s awareness or simply not owned by that person. ○ EXAMPLE: Stomach is part of the organismic self, but it is not likely to be a part of one’s self-concept unless it malfunctions and causes concern ● Once people form their self-concept, they find change and significant learning quite difficult.
○ Experiences that are inconsistent with their self-concept are either denied or accepted only in distorted forms. The Ideal Self ● One’s view of the self as one wishes to be ● Contains all those attributes that people aspire to possess. ● Wide gap between the ideal self and self-concept indicates incongruence and unhealthy personality. ● Psychologically healthy individuals perceive little discrepancy between their self-concept and what they ideally would like to be.
Awareness (AKI) ● Is the symbolic representation of some portion of our experience ● Without awareness self-concept and the ideal self would not exist Levels of Awareness ● 3 levels ○ 1st: there are experienced events that may be either ignored or denied ○ 2nd: some experiences are accurately symbolized and freely itted to the self-structure ○ 3rd: involved experiences that are perceived in a distorted form (we reshape or distort the experience for it to be consistent with our view of self) Denial of Positive Experiences ● Not only negative or derogatory experiences that are distorted or denied to awareness; many people also have difficulty in accepting positive and genuine compliments ● They may be distorted because the person distrusts the giver, or they may be denied because the recipient does not feel deserving of them ● A compliment from another also implies the right of that person to criticize or condemn, and thus the compliment carries an implied threat Becoming a Person (AKI) ● First, an individual must make (positive or negative) with another person ○ In order to survive, an infant must experience some from a parent or caregiver
● As children (or adults) become aware that another person has some measure of regard for them, they begin to value positive regard and devalue negative regard ○ That is, the person develops a need for positive regard (love, liked, or accepted by another person) ○ If we perceive that other/significant others value us, then our need for positive regard is at least partially satisfied ● Positive regard is a prerequisite for positive self-regard (defined as the experience of prizing or valuing one’s self) ● Once positive self-regard is established, it becomes independent of the continual need to be loved ● The source of positive self-regard, then, lies in the positive regard we receive from others ○ But once established, it is autonomous and self-perpetuating Barriers to Psychological Health - Not everyone becomes a healthy person. Most people experience the four barriers to psychological health. Conditions of Worth - People perceive that their parents, peers or partners love and accept them only if they meet those people’s expectations and approval. - Arises when the positive regard of a significant other is conditional, when the individual feels that in some respects he/she is prized and in others not - Criterion by which we accept or reject our experiences - If we see that others accept us regardless of our actions, then we come to believe that we are prized unconditionally. - If we perceive that some of our behaviors are approved and some disapproved, then we see that our worth is conditional. - We introject the values of others - External Evaluations: our perceptions of other people’s view of us - Prevent us from being completely open to our own experiences - Example: We may reject pleasurable experiences because we believe that other people do not approve of them Incongruence - Organism and the self are two separate entities (may or may not be congruent with one another)
-
Psychological disequilibrium : begins when we fail to recognize our organismic experiences as self-experiences Source of psychological disorders Conditions of Worth → Self-concept → Incongruence
A. Vulnerability - The greater the incongruence between our perceived self/self-concept and our organismic experience, the more valuable we are. - People are vulnerable when they are unaware of the discrepancy between their organismic self and their significant experience - Often behave in ways that are incomprehensible not only to others but also to themselves B. Anxiety and Threat - Anxiety: state of uneasiness or tension whose cause is unknown - When we become dimly aware that the discrepancy between our organismic experience and our self-concept may become conscious - As we become more aware of the incongruence between our organismic experience and our self-concept, our anxiety evolves into threat - Represent steps toward psychological health - These two signal to us that our organismic experience is inconsistent with our self-concept Defensiveness (ROSE) - In order to prevent the inconsistency between our organismic experience and our perceived self, we react in a defensive manner - Defensiveness - the protection of self-concept against anxiety and threat by the denial or distortion of experiences inconsistent with it - When our experiences is inconsistent with one part of our self-concept, we will behave in a defensive manner in order to protect the current structure of our self-concept - 2 chief defenses: distortion and denial - Distortion - We misinterpret an experience in order to fit it into some aspect of our self-concept
-
-
-
-
-
-
We perceive the experience in awareness, but we fail to understand its true meaning - Denial - We refuse to perceive an experience in awareness, or at least we keep some aspect of it from reaching symbolization - Not as common as distortion because most experiences can be twisted or reshaped to fit the current self-concept ● Distortion and denial serve the same purpose: they keep our perception of our organismic experiences consistent with our self-concept which allows us to block out experiences that otherwise would cause unpleasant anxiety or threat Disorganization (ROSE) Most people engage in defensive behavior, but sometimes defenses fail and behavior becomes disorganized or psychotic We must trace the course of disorganized behavior, which has the same origins as normal defensive behavior, namely a discrepancy between people’s organismic experience and their view of self. Denial and distortion are adequate to keep normal people from recognizing this discrepancy, but when the incongruence between people’s perceived self and their organismic experience is either too obvious or occurs too suddenly to be denied or distorted, their behavior becomes disorganized. Disorganization can occur suddenly, or it can take place gradually over a long period of time. In a state of disorganization, people sometimes behave consistently with their organismic experience and sometimes in accordance with their shattered self-concept - Example 1:First case is a previously prudish and proper woman who suddenly begins to use language explicitly sexual and scatological - Example 2: The second case can be illustrated by a man who, because his self-concept is no longer a gestalt or unied whole, begins to behave in a confused, inconsistent, and totally unpredictable manner. In both cases, behavior is still consistent with the self-concept, but the self-concept has been broken and thus the behavior appears bizarre and confusing. Rogers always remained uncomfortable with the “neurotic” and “psychotic,” preferring instead to speak of “defensive” and “disorganized” behaviors, that more accurately convey the idea that psychological maladjustment is on a continuum from the slightest discrepancy between self and experience to the most incongruent
PSYCHOTHERAPY Conditions (ELAINE) In order for therapeutic growth to take place, the following conditions are necessary and sufficient: 1. Anxious or vulnerable client must come into with a congruent therapist who also possesses empathy and unconditional positive regard for that client. 2. The client must perceive these characteristics in the therapist. 3. There must be some duration for the between client and therapist Note: The first and third conditions are present with nearly any psychotherapy ● Client-centered therapy: unique in its insistence that the conditions of counselor congruence, unconditional positive regard, and empathic listening are both necessary and sufficient. - Congruence: general quality possessed by the therapist - Unconditional positive regard & emphatic listening: specific feelings or attitudes that the therapist has for an individual client Counselor Congruence ( ELAINE) - Congruence: exists when a person’s organismic experiences are matched by an awareness of them and by ability and willingness to openly express these feelings - To be real or genuine - To be whole or integrated - To be what one truly is - Congruent therapist: First necessary and sufficient condition for therapeutic change - Congruent counselor: a complete human being with feelings of joy, anger, frustration, confusion - Despite being constantly exposed to new organismic experiences, they accept these experiences into awareness -> psychological growth - They wear no mask, do not attempt to fake a pleasant facade,and avoid any pretense of friendliness and affection when these emotions are no truly felt - They are able to match feelings with awareness and both with honest expression - Congruence involves: feelings, awareness, expression
-
Incongruence can arise from either of the two points dividing these three experiences. 1. Breakdown between feelings and awareness: a person may be feeling angry, and the anger may be obvious to others; but the angry person is unaware of the feeling. 2. Discrepancy between awareness of an experience and the ability or willingness to express it to another: “I know I’m feeling bored by what is being said, but I don’t dare verbalize my disinterest because my client will think that I am not a good therapist” ● Rogers: therapists will be more effective if they communicate genuine feelings, even when those feelings are negative or threatening ● To do otherwise would be dishonest, clients will detect any significant indicators of incongruence. ● Rogers: Although congruence is a necessary ingredient in successful therapy, it is not necessary for a therapist to be congruent in all relationships outside the therapeutic process. ○ One can be less than perfect yet an effective psychotherapist ○ One need not be absolutely congruent in order to facilitate some growth within a client ○ Different degrees of congruence exist with unconditional positive regard and empathic listening. ● THE MORE THE CLIENT PERCEIVES EACH OF THESE QUALITIES AS CHARACTERIZING THE THERAPIST, THE MORE SUCCESSFUL WILL BE THE THERAPEUTIC PROCESS. Unconditional Positive Regard ( KATHLEEN) ● Unconditional - positive regard is no longer dependent on specific client behaviors and does not have to be continually earned. ● Positive - indicates that the direction of the relationship is toward warm and caring feelings ● Regard - there is a close relationship and that the therapist sees the client as an important person ● Positive regard - the need to be liked, prized, or accepted by another person. ● Unconditional positive regard - need that exists without any conditions or qualifications
○ “experiencing a warm, positive and accepting attitude toward what is the client” ○ without possessiveness, without evaluations, and without reservations ○ shows a nonpossessive warmth and acceptance, not an effusive, effervescent persona. ■ caring for others without smothering or owning that person. ■ allowing others you care to be autonomous and independent of your evaluations and restrictions. ■ respecting that others have their own feelings and opinions ■ letting the other person be its own self by making it decide for itself ■ in short, mind your own business at may sarili siyang kakayahan sa buhay nya :3 ● Therapists: ■ Must be client-centered and actively involved in a relationship with the client. ■ they must accept and prize their clients without any restrictions or reservations and without regard to the clients’ behavior. ■ may value some client behaviors more than others ■ positive regard must remain constant and unwavering. ■ Must not evaluate clients, nor do they accept one action and reject another. ● External evaluation leads to clients’ defensiveness and prevents psychological growth.
Empathic Listening (KATHLEEN) ● Necessary and sufficient of psychological growth ● Empathy - exists when therapists accurately sense the feelings of their clients and are able to communicate these perceptions - Being able to enter the world of feelings without prejudice, projection, or evaluation. - Roger: “means temporarily living in the other’s life, moving about in it delicately without making judgments” - does not involve interpreting clients’ meanings or uncovering their unconscious feelings, procedures that would entail an external frame of reference and a threat to clients. - suggests that a therapist sees things from the client’s point of view and that the client feels safe and unthreatened.
-
effective because it enables clients to listen to themselves and, in effect, become their own therapists.
EMPATHY
SYMPATHY
A feeling with a client
A feeling for a client Never therapeutic Stems from external evaluation Leads to client’s self-pity - Threatens positive self-concept - Creates self-structure disequilibrium
● Empathic listening - a powerful tool that facilitates personal growth within the client. ● Empathy in effect - When persons are perceptively understood, they find themselves coming in closer touch with a wider range of their experiencing. - Find people which they can turn for guidance in understanding themselves and directing their behavior. - If accurate and deep, they may also be able to unblock a flow of experiencing and permit it to run its uninhibited course. ● An empathic therapist ○ do not take empathy for granted ○ checks the accuracy of their sensings by trying them out on the client. ○ does not have the same feelings as the client ○ does not feel anger, frustration, confusion, resentment, or sexual attraction at the same time a client experiences them. ○ experiences the depth of the client’s feeling while permitting the client to be a separate person. ○ has an emotional as well as a cognitive reaction to a client’s feelings not belonging to the therapist, but the feelings belong to the client ○ does not take ownership of a client’s experiences ○ able to convey to the client an understanding of what it means to be the client at that particular moment Process If the conditions of therapist congruence, unconditional positive regard, and empathy are present, then the process of therapeutic change will be set in motion.
Stages of Therapeutic Change
The process of constructive personality change can be placed on a continuum from most
defensive to most integrated. Rogers (1961) arbitrarily divided this continuum into seven stages. Stage 1
● ●
characterized by an unwillingness to communicate anything about oneself. People at this stage ordinarily do not seek help, but if for some reason they come to therapy, they are extremely rigid and resistant to change.
Stage 2
● ●
clients become slightly less rigid. They discuss external events and other people, but they still disown or fail to recognize their own feelings. (feelings were such objective phenomena).
Stage 3
● ●
more freely talk about self, although still as an object. Clients talk about feelings and emotions in the past or future tense and avoid present feelings. vaguely perceive that they can make personal choices, and deny individual responsibility for most of their decisions
● Stage 4
● ● ●
●
Stage 5
● ● ●
● Stage 6
● ● ● ● ●
begin to talk of deep feelings but not ones presently felt. They deny or distort experiences, although they may have some dim recognition that they are capable of feeling emotions in the present. They begin to question some values that have been introjected from others, and they start to see the incongruence between their perceived self and their organismic experience. They accept more freedom and responsibility than they did in Stage 3 and begin to tentatively allow themselves to become involved in a relationship with the therapist. they have begun to undergo significant change and growth. They can express feelings in the present, although they have not yet accurately symbolized those feelings. They are beginning to rely on an internal locus of evaluation for their feelings and to make fresh and new discoveries about themselves. They also experience a greater differentiation of feelings and develop more appreciation for nuances among them. In addition, they begin to make their own decisions and to accept responsibility for their choices experience dramatic growth and an irreversible movement toward becoming fully functioning or self-actualizing. They freely allow into awareness those experiences that they had previously denied or distorted. They become more congruent and are able to match their present experiences with awareness and with open expression. They no longer evaluate their own behavior from an external viewpoint but rely on their organismic self as the criterion for evaluating experiences. They begin to develop unconditional self-regard, which means that they have a feeling of genuine caring and affection for the person they are
●
Stage 7
● ● ● ●
●
becoming. An interesting concomitant to this stage is a physiological loosening. These people experience their whole organismic self, as their muscles relax, tears flow, circulation improves, and physical symptoms disappear. occur outside the therapeutic encounter, because growth at Stage 6 seems to be irreversible. “persons of tomorrow” They are able to generalize their in-therapy experiences to their world beyond therapy. They possess the confidence to be themselves at all times, to own and to feel deeply the totality of their experiences, and to live those experiences in the present. People receive pleasure in knowing that these evaluations are fluid and that change and growth will continue. In addition, they become congruent, possess unconditional positive self-regard, and are able to be loving and empathic toward others.
Theoretical Explanation for Change When people come to experience themselves as prized and unconditionally accepted, they realize, perhaps for the first time, that they are lovable. ● As clients perceive that they are emphatically understood, they are freed to listen to themselves more accurately, to have empathy for their own feelings. ● As a consequence, when these persons come to prize themselves and to accurately understand themselves, their perceived self becomes more congruent with their organismic experiences. ● They now possess the same three therapeutic characteristics as any effective helper, and in effect, they become their own therapist. Outcomes (MARION) ● The most basic outcome of successful client-centered therapy is a congruent client ○ less defensive and more open to experience ○ have a clearer picture of themselves and a more realistic view of the world ○ Can assimilate experiences into the self on the symbolic level ○ they are more effective in solving problems ○ they have a higher level of positive self-regard. ● More realistic ○ Accurate view of potentials which narrows the gap between ideal and actual self ● less physiological and psychological tension
● ● ● ●
More accepting of others more mature, likeable, and socialized Their genuineness, positive self-regard and empathic ununderstanding are extended beyond therapy, and they become better able to participate in other growth-facilitating relationships
THE PERSON OF TOMORROW - If the three necessary and sufficient therapeutic conditions are optimal, a person of tomorrow will emerge. - Person of tomorrow = fully functioning people; psychologically healthy individuals - There are eight characteristics of a person of tomorrow: (1) MORE ADAPTABLE ❏ More likely to survive from an evolutionary perspective ❏ Realization that conformity and adjustment to a fixed condition have little long-term survival value (2) OPEN TO THEIR EXPERIENCES
❏ Do not deny or distort experiences ❏ All internal and external stimuli are freely received by the self ❏ Listen to themselves and hear their emotions e.g. joy, anger, fear (3) TRUST IN THEIR ORGANISMIC SELVES ❏ ❏ ❏ ❏
Do not depend on others for guidance Use own experiences as best criteria when making choices Trust their own inner feelings when making decisions Take into consideration the rights and feelings of others which they see clearly when making decisions
(4) LIVE FULLY IN THE MOMENT ❏ See each experience with a new freshness and appreciate it fully in the present ❏ Existential tendency: the tendency to live in the moment ❏ No need to deceive themselves and no reason to impress others ❏ No preconceptions about how the world should be ❏ Live the experience without prejudice of prior expectations (5) EXPERIENCE HARMONIOUS RELATIONS WITH OTHERS ❏ ❏ ❏ ❏
Feel no need to be liked or loved by everyone Know that they are unconditionally prized and accepted by someone Authentic in their relations with others Show care towards others without prejudice
(6) MORE INTEGRATED ❏ ❏ ❏ ❏ ❏
More whole individual See differences clearly Bridge the gap between real self and ideal self Present no facades to other people Openly express whatever feelings they are experiencing
(7) HAS BASIC TRUST OF HUMAN NATURE ❏ Would not harm others for personal gain ❏ Would care about others and ready to offer help when needed ❏ Do not strike out unreasonably against others
❏ Channel aggression in appropriate directions (8) ENJOY A GREATER RICHNESS OF LIFE ❏ Feel more deeply than others ❏ Live in the present and participate in the moment more fully than others PHILOSOPHY OF SCIENCE (JORDAN) ●
Science begins and ends with the subjective experience, everything in between must be objective and empirical.
What a scientist should be ●
● ●
Scientists must have characteristics of the person of tomorrow ○ look within ○ be in tune with internal feelings and values ○ be intuitive and creative ○ be open to experiences ○ welcome change ○ have a fresh outlook ○ possess a solid trust in themselves scientists should care for newly born ideas and nurture them lovingly scientists should be completely involved in the phenomena being studied ○ ex. People who conduct research on psychotherapy must first have had long careers as therapists.
How Science Happens ●
●
●
An intuitive scientist perceives patterns among phenomena. (may be too vague to communicate, but are nourished by a scientist to become a testable hypothesis) ○ hypothesis comes from an open-minded scientist, not stereotypical thoughts Methodology - must be rigorously controlled, empirical, and objective ○ precise methods prevent self-deception and from intentionally or unintentionally manipulating the observations (only the method of science that is precise and objective, not science itself) Scientist communicates findings from that method to others, ○ communication itself is subjective: The people receiving the communication bring their own degrees of open-mindedness or defensiveness into this process.
THE CHICAGO STUDIES (ANDREA) ● Rogers did not permit methodology to dictate the nature of his research ○ Allowed the problem to take precedence over methodology and measurement ○ They began by sensing vague impressions from clinical experience and gradually forming these into testable hypotheses ● Purpose: investigate both the process and the outcomes of client-centered therapy Hypotheses (ANDREA) ● States that all persons have within themselves the capacity, either active or latent, for self-understanding as well as the capacity and tendency to move in the direction of self-actualization and maturity. ● During therapy, clients would assimilate into their self-concepts those feelings and experiences previously denied to awareness. ● During and after therapy, the discrepancy between real self and ideal self would diminish and behavior of clients would be more socialized, more self-accepting, and more accepting of others. Method (ANDREA) ● Difficulty in selecting measuring instruments ○ Because the hypothesis dictates that subtle subjective personality changes should be measured objectively ● Used Thematic Apperception Test (TAT) ○ Projective personality test developed by Henry Murray ○ Used to test hypothesis that called for a standard clinical diagnosis ● Used Self-Other Attitude Scale (S-O Scale) ○ Instrument compiled at the Counseling Center from several earlier sources ○ Measures antidemocratic trends and ethnocentrism ● Used Willoughby Emotional Maturity Scale (E-M Scale) ○ Used to compare descriptions of clients’ behavior and emotional maturity as seen by two close friends and the clients themselves ● Used Q sort technique ○ Developed by William Stephenson ○ Measures changes from the client’s point of view ○ Begins with a universe of 100 self-referent statements printed on 3x5 cards
○ Participants are requested to sort into nine piles from “most like me” to “least like me” ○ Resulting distribution approximates a normal curve and allows for stat analysis ○ Participants were also requested to sort the cards to describe their self, their ideal self, and the ordinary person ● Participants ○ 18 men and 11 women who had sought therapy at Counseling Center ○ Called the experimental or therapy group ○ Received at least 6 therapeutic interviews and each session was recorded and transcibed ■ A procedure Rogers pioneered ● Methods of Control First Control ○ Own-Control or Wait Group ■ Participants waited 60 days before they would receive therapy ■ In order to determine if motivation to change rather than the therapy itself might cause people to get better ○ No-Wait Group ■ Received therapy immediately Second Control ○ Consisted of a separate group of “normals” ■ This comparison group allowed researchers to determine the effects of such variables as age of time, knowledge that one is part of an experiment (placebo effect), and impact of repeated testing ■ Divided into wait group and no-wait group
● Both were tested 4 times ○ At the beginning of 60-day wait period ○ Prior to therapy ○ Immediately after therapy ○ After a 6-12-months follow-up period Findings (LEI) Summary of Results (LEI)
Related Documents c2h70

Carl Rogers 1o2q6u
December 2019 76
Mapas De Carl Rogers 4k2j13
September 2021 0
Carl Rogers El Humanismo 3w4p3f
February 2023 0
Carl Rogers Humanisme 47401q
May 2023 0
Carl Rogers- Fred Zimring 6y2ff
December 2021 0
Psicologia Humanista Carl Rogers 6m13w
October 2022 0More Documents from "Aiden Lee" 2f5f4t
Carl Rogers _ Person-centered Theory.pdf 62h6u
July 2022 0
November 2019 65
Identifikasi-bahaya-penilaian-risiko-skala-prioritas-pengendalian-risiko.xlsx 5e745
April 2020 8
6g3p1u
November 2019 55
Ferry Timetable 16115p
July 2022 0