Slide Ortho Tibia And Fibula Ppt 3r275j
This document was ed by and they confirmed that they have the permission to share it. If you are author or own the copyright of this book, please report to us by using this report form. Report 2z6p3t
Overview 5o1f4z
& View Slide Ortho Tibia And Fibula Ppt as PDF for free.
More details 6z3438
- Words: 708
- Pages: 25
PATIENT IDENTITY Name :B Age : 44 years old Sex : Male Date of ission :August 23rd, 2015 at 16.30 RM number : 723290
HISTORY TAKING Chief Complaint: Pain at right leg Suffered since 22 hours before being itted to Wahidin General Hospital Patient was riding a motorcycle when he fell down due to loss of balance Patient’s right leg first came into with the ground. Vomitting (-) nausea (-) Prior treatment : Pangkep Hospital
PRIMARY SURVEY Airway : Clear Breathing: RR = 20x/min, regular, spontaneous, thoracoabdominal type, symmetrical. Circulation: BP = 120/70 mmHg,HR = 80 x/min regular, strong. Disability : GCS 15 (E4V5M6),isochoric pupil, Ø : 2,5 mm, light reflex +/+ Exposure : T = 36,70 C (axilla)
SECONDARY SURVEY Localized status : Right Leg region Look:
Deformity (+), swelling (+), hematoma (+), Wound (-) Feel : tenderness (+) Move: Active and ive motions of the knee are limited due to pain Active and ive motions of the ankle are limited due to pain NVD : Good sensibility, dorsalis pedis and tibialis anterior pulses are palpable, CRT <2”,
CLINICAL FINDINGS
LEG LENGTH DISCREPANCY Right
Left
ALL
86
87
TLL
82
83
LLD
1 cm
LABORATORY FINDINGS WBC : 15.400/ ul RBC : 5.000.000/ ul HBG : 14.7 g/dl HCT : 43 % PLT : 233.000/mm3 CT : 7’30’’ BT : 2’30’’ HBsAg : Non reactive
X-RAY RIGHT CRURIS
AP View
Lateral View
DIAGNOSIS Closed fracture 1/3 distal right tibia Closed fracture 1/3 distal right fibula
MANAGEMENT IVFD
RL Analgesic Report to Orthopaedic senior, advice: Apply
Plan
boot slab left lower limb
for ORIF Tibia & Fibula
RESUME • A Boy 44 years old came to the hospital with chief complaint pain at the left leg, suffered since 22 hours before itted to Hospital. • At the anterolateral aspect, there is haematom and edema.The region was tenderness on palpation, with unknown active and ive motion of knee t and ankle t due to pain. Sensibility is good and dorsalis pedis artery is palpable, CRT <2” . • laboratory findings are within normal limit, • From radiology finding (X-Ray cruris dextra AP/Lateral) there is closed fracture 1/3 distal of right tibia and fibula.
Discussion
TIBIA AND FIBULA
Thompson, J. Netter’s Concise Orthopaedic Anatomy, 2nd Ed. Elsevier Saunders, 2010.
NETTER’S CONCISE ORTHOPAEDIC ANATOMY, P. 316
NETTER’S CONCISE ORTHOPAEDIC ANATOMY, P. 317
NETTER’S CONCISE ORTHOPAEDIC ANATOMY, P. 318
TYPES OF FRACTURES
Thompson, J. Netter’s Concise Orthopaedic Anatomy, 2nd Ed. Elsevier Saunders, 2010.
Clinical features
Diagnosis
Anamnesis
Physical examination
X- ray, with anteriorposterior and lateral view
Laboratory examination
Oedema Hematoma
Tenderness at the fracture site. Decreased range of motion at the ankle or knee, depending on the location of the fracture If fracture is displaced, a deformity may be noted
Appley’s . Sistem Of orthopaedis & fracture,8th edition.
TSCHERNE’S CLASSIFICATION OF SKIN LESION IN CLOSED FRACTURES Grade 0
Injury from indirect forces with negligible soft tissue damage
Grade I
Closed fracture caused by low-moderate energy mechanisms, with superficial abrasions or contusions of soft tissues overlying the fracture
Grade II
Closed fracture with significant muscle contusion, with possible deep, contaminated skin abrasions associated with moderate to severe energy mechanisms and skeletal injury; high risk for compartment syndrome
Grade III
Extensive crushing of soft tissues, with subcutaneous degloving or avulsion, with arterial disruption or established compartment syndrome
TREATMENT
Conservative Closed reduction • Apply long leg cast • Functional bracing with Early weight-bearing • Pain medication if needed •
TREATMENT
Operative
Internal Fixation External Fixation
DEFINITIVE TREATMENT Open Reduction Internal Fixation Indication of ORIF in this patient is : ORIF Tibia Acceptable fracture reduction is not indicated anymore in this patient ORIF Fibula There’s fracture at 3 cm from syndesmosis at X-Ray findings Advantage Adequate reduction Early movement Disadvantage Increase risk of infection, skin problem A high degree of surgical technique and facilities are essential
COMPLICATIONS Early complications
Late complication
Neurovascular injury
Malunion, delay union, nonunion
Compartment syndrome
t stiffness infection
HISTORY TAKING Chief Complaint: Pain at right leg Suffered since 22 hours before being itted to Wahidin General Hospital Patient was riding a motorcycle when he fell down due to loss of balance Patient’s right leg first came into with the ground. Vomitting (-) nausea (-) Prior treatment : Pangkep Hospital
PRIMARY SURVEY Airway : Clear Breathing: RR = 20x/min, regular, spontaneous, thoracoabdominal type, symmetrical. Circulation: BP = 120/70 mmHg,HR = 80 x/min regular, strong. Disability : GCS 15 (E4V5M6),isochoric pupil, Ø : 2,5 mm, light reflex +/+ Exposure : T = 36,70 C (axilla)
SECONDARY SURVEY Localized status : Right Leg region Look:
Deformity (+), swelling (+), hematoma (+), Wound (-) Feel : tenderness (+) Move: Active and ive motions of the knee are limited due to pain Active and ive motions of the ankle are limited due to pain NVD : Good sensibility, dorsalis pedis and tibialis anterior pulses are palpable, CRT <2”,
CLINICAL FINDINGS
LEG LENGTH DISCREPANCY Right
Left
ALL
86
87
TLL
82
83
LLD
1 cm
LABORATORY FINDINGS WBC : 15.400/ ul RBC : 5.000.000/ ul HBG : 14.7 g/dl HCT : 43 % PLT : 233.000/mm3 CT : 7’30’’ BT : 2’30’’ HBsAg : Non reactive
X-RAY RIGHT CRURIS
AP View
Lateral View
DIAGNOSIS Closed fracture 1/3 distal right tibia Closed fracture 1/3 distal right fibula
MANAGEMENT IVFD
RL Analgesic Report to Orthopaedic senior, advice: Apply
Plan
boot slab left lower limb
for ORIF Tibia & Fibula
RESUME • A Boy 44 years old came to the hospital with chief complaint pain at the left leg, suffered since 22 hours before itted to Hospital. • At the anterolateral aspect, there is haematom and edema.The region was tenderness on palpation, with unknown active and ive motion of knee t and ankle t due to pain. Sensibility is good and dorsalis pedis artery is palpable, CRT <2” . • laboratory findings are within normal limit, • From radiology finding (X-Ray cruris dextra AP/Lateral) there is closed fracture 1/3 distal of right tibia and fibula.
Discussion
TIBIA AND FIBULA
Thompson, J. Netter’s Concise Orthopaedic Anatomy, 2nd Ed. Elsevier Saunders, 2010.
NETTER’S CONCISE ORTHOPAEDIC ANATOMY, P. 316
NETTER’S CONCISE ORTHOPAEDIC ANATOMY, P. 317
NETTER’S CONCISE ORTHOPAEDIC ANATOMY, P. 318
TYPES OF FRACTURES
Thompson, J. Netter’s Concise Orthopaedic Anatomy, 2nd Ed. Elsevier Saunders, 2010.
Clinical features
Diagnosis
Anamnesis
Physical examination
X- ray, with anteriorposterior and lateral view
Laboratory examination
Oedema Hematoma
Tenderness at the fracture site. Decreased range of motion at the ankle or knee, depending on the location of the fracture If fracture is displaced, a deformity may be noted
Appley’s . Sistem Of orthopaedis & fracture,8th edition.
TSCHERNE’S CLASSIFICATION OF SKIN LESION IN CLOSED FRACTURES Grade 0
Injury from indirect forces with negligible soft tissue damage
Grade I
Closed fracture caused by low-moderate energy mechanisms, with superficial abrasions or contusions of soft tissues overlying the fracture
Grade II
Closed fracture with significant muscle contusion, with possible deep, contaminated skin abrasions associated with moderate to severe energy mechanisms and skeletal injury; high risk for compartment syndrome
Grade III
Extensive crushing of soft tissues, with subcutaneous degloving or avulsion, with arterial disruption or established compartment syndrome
TREATMENT
Conservative Closed reduction • Apply long leg cast • Functional bracing with Early weight-bearing • Pain medication if needed •
TREATMENT
Operative
Internal Fixation External Fixation
DEFINITIVE TREATMENT Open Reduction Internal Fixation Indication of ORIF in this patient is : ORIF Tibia Acceptable fracture reduction is not indicated anymore in this patient ORIF Fibula There’s fracture at 3 cm from syndesmosis at X-Ray findings Advantage Adequate reduction Early movement Disadvantage Increase risk of infection, skin problem A high degree of surgical technique and facilities are essential
COMPLICATIONS Early complications
Late complication
Neurovascular injury
Malunion, delay union, nonunion
Compartment syndrome
t stiffness infection
Related Documents c2h70
Slide Ortho Tibia And Fibula Ppt 3r275j
March 2021 0
Askep Fraktur Tibia Fibula 2fv3j
November 2019 74
Fraktur Tibia Fibula 6b6g6h
October 2019 61
Anatomy And Physiology Of Tibia And Fibula 133e1i
November 2019 17
Case Report Cl Fracture Tibia Fibula 5s3r72
January 2021 0
Laporan Kasus Fraktur Radius, Tibia Dan Fibula 663h5g
April 2020 17More Documents from "leonard" 4w4t3s

Mb-42 Bender 5b6c1p
December 2021 0
Dp8 Manual 2wp46
December 2019 95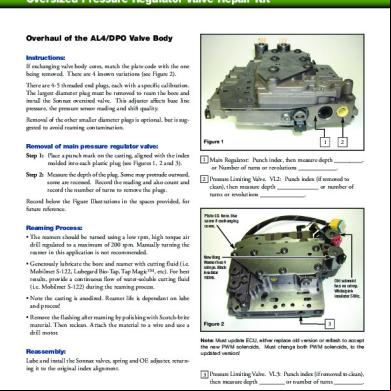
Al4 Dpo Peugeot, Renault, Citroen Overhaul Al4 Dpo Valve Body Tech Line Pressure Problem And Transmission Overheating. 2n6b6z
November 2021 0
Tb-60 Top Bender 522c28
October 2019 95
Slide Ortho Tibia And Fibula Ppt 3r275j
March 2021 0