Operating Room Techniques md2q
This document was ed by and they confirmed that they have the permission to share it. If you are author or own the copyright of this book, please report to us by using this report form. Report 2z6p3t
Overview 5o1f4z
& View Operating Room Techniques as PDF for free.
More details 6z3438
- Words: 1,633
- Pages: 33
PERIOPERATIVE NURSING
Venus Sofia J. Balatero, RN, USRN
Perioperative Nursing • Perioperative nursing is not just "technical work anyone can do". Perioperative nurses are skilled, knowledgeable RNs that care for patients before, during, and after surgery. • The fundamental nursing values (knowledge, skills, and judgment) are ever present and are the basis of the quality of care that surgical patients have relied on and can expect.
Perioperative Nursing
•The patient is the center of the sterile field
Perioperative Nursing The OR team usually consists of: • Surgeon: Scrubbed and in surgical attire to perform the surgery • Anesthesia provider: Masked and in clean scrub attire to ister the anesthesia - During the procedure the anesthesiologist monitors the patient’s vital signs and is responsible for keeping the surgeon aware of the patient’s condition. The anesthesiologist determines when the patient may be moved to the post anesthesia recovery stretcher after the surgical procedure has been completed. This person usually checks the patient’s airway and vital signs before taking the patient to the post anesthesia recovery room.
Perioperative Nursing The OR team usually consists of: • Surgical assistant (first assistant):
Can be another physician, a nurse, or physician’s assistant (PA) who is scrubbed, in sterile attire, and assists the surgeon to ligate, suction, and suture • Scrub nurse: Scrubbed and in sterile attire; prepares the instrument tray and es the instruments, sponges, needles, and sutures to the surgeon • Circulating nurse: In clean scrub attire and mask; assure that sterility is maintained at all times; obtains supplies, delivers materials, pours solutions, handles specimens, positions the client and surgical drapes, and disposes of soiled items
Perioperative Nursing
• PHASES –Perioperative –Intraoperative –Postoperative
Perioperative Nursing • PREOPERATIVE PHASE – Begins when the decision is made to undergo surgical intervention and it ends when the patient is transferred to the OR bed – During this phase, the perioperative nurse performs the assessment, determines the nursing diagnoses, identifies potential outcomes and develops a plan of care – The perioperative nurse plans, prioritizes, and initiates the patient care necessary for the attainment of the desired outcomes
Perioperative Nursing • INTRAOPERATIVE PHASE -Begins with the placement of the patient on the OR bed and continues until the patient is itted to a postprocedure or postoperative area -Implementation of the plan and evaluation of care continues during this phase.
Perioperative Nursing • POSTOPERATIVE PHASE -Begins with ission of the patient to a postprocedure or postanethesia area, which may be a postanesthesia care unit (PACU) or an intensive care unit (ICU). -Patients itted to the facility on an ambulatory 1-day-stay basis may return to the ambulatory unit. As indicated by his condition, the patient will transfer from the immediate postoperative patient care division for progressive stages of self-care on a surgical unit before being discharged from the hospital. -The postoperative phase ends when the surgeon discontinues follow-up care -Evaluation, the sixth component of the nursing process, is completed during this phase
Perioperative Nursing Phase Preoperative
From
To
Decision for surgical Transfer to intervention Operating Room
Intraoperative Received in Operating Room
ission to Recovery Room
Postoperative ission to recovery Room
Follow-up Evaluation
Type of Surgery acc. to URGENCY Type of Surgery
Optional Elective Planned/ Required Urgent/ Imperative Emergency
Time requirement for surgery At the preference of patient; surgery not needed At the convenience of patient as failure to have surgery is not catastrophic Within a few weeks as surgery is important Within 24-48 hours
Example Cosmetic surgery Liposuction Excision of superficial cyst Cataract extraction Cancer surgery
Immediately without delay to Intestinal maintain life or organ, Obstruction remove damage, stop bleeding
Type of Surgery acc. to PURPOSE Type of Surgery
Diagnostic Exploratory
Purpose
Example
To confirm diagnosis
Excision and biopsy To estimate the extent of the Exploratory disease and confirm Laparotomy diagnosis as well
Curative -Ablative Removal of diseased organ -Constructive Repair of congenital defects -Reconstructive Restoration of damaged organ Palliative Relieves symptom but does not cure the disease
Hysterectomy Repair of cleft lip or palate Episiorrhapy Rhizotomy and chordotomy (for pain relief)
Type of Surgery acc. to SERIOUSNESS Type of Surgery
Minor Major
Extent of Surgery Surgery that involves minimal (few) complications and minimal blood loss Extensive surgery that involves serious risk and complications (and loss of blood) as it involves major organs
Sterile Technique
Sterile Technique • Strict adherence to sound principles of sterile technique and recommended practices is mandatory for the safety of the patient. • This adherence reflects one’s surgical conscience. • Principles remain the same; it is the degree of adherence to them that varies.
Principles of Sterile Technique • Sterile persons have scrubbed and are gowned and gloved; unsterile person have not. • Only Sterile Items Are Used Within the Sterile Field. • If you are in doubt about the sterility of anything, consider it not sterile. • Gowns Are Considered Sterile Only from the Waist to Shoulder Level Front and the Sleeves • Tables Are Sterile Only at Table Level
Principles of Sterile Technique • Persons Who Are Sterile Touch Only Sterile Items of Areas; Persons Who Are Not Sterile Touch Only Unsterile Items or Areas • Unsterile Persons Avoid Reaching over a Sterile Field; Person Avoid Leaning over an Unsterile Area • Edges of anything that encloses Sterile Contents are Considered Unsterile • Sterile Field is Created as close as Possible to time of Use
Principles of Sterile Technique • Sterile Areas are Continuously Kept in View • Sterile Persons Keep well within the Sterile Area - They do not walk around or go outside room - Sterile Persons keep wit Sterile Areas to a Minimum • Unsterile Persons Avoid Sterile Areas • Destruction of Integrity of Microbial Barriers Results in Contamination - Strike-through is soaking of moisture through unsterile layers to sterile layers or vice-versa. • Microorganism Must be kept to an Inducible Minimum
Perioperative Nursing • PATIENTS SKIN PREP - done after patient has been anesthetized and positioned on the operating table, skin of the operative site and extensive area surrounding it is mechanically cleansed again with an antiseptic agent immediately prior to draping
Perioperative Nursing
• PATIENTS SKIN PREP - Responsibility: The first assistant is the person who scrubs the patient after he has scrubbed his own hands and arms
Perioperative Nursing • PATIENTS SKIN PREP - Scrub skin, starting at site if incision, with a circular motion or over widening circles to the periphery. Use enough pressure and friction to remove dirt and microorganisms from skin and pores. - Discard sponge after reaching periphery. Never bring a soiled sponge back toward center of area
Perioperative Nursing • Contaminated Areas within the Operative Field: - Umbilicus, stoma, draining sinuses, skin ulcer, vagina, anus, colostomy, (In all contaminated areas, follow general rule of scrubbing the most contaminated area last of with a separated sponge
Layers of Tissue The five main layers of abdominal tissue from the outer most are: • Skin • Subcutaneous • Fascia • Muscle • Peritoneum
PACU
PACU • The post anesthesia recovery room is rarely called an intensive care unite, but it is. • Everyday is a real challenge to PACU nurses because many kinds of situations occur. They are expected to have good knowledge of both medical and surgical procedures because they care for patients with all types of medical and surgical problems. The nurses must be calm and in full command of the situation but know their limitations • The PACU nurse works under the direction of the anesthesiologist or surgeon. The nurse must carry out simultaneously four assignments: - Observation of the patient - Evaluation of those observations - Performance of the necessary treatment - Reporting and recording observations and treatment • Total care of the patient requires both-in-depth study and experience in post anesthesia recovery nursing.
PACU • The PACU nurse must totally evaluate the patient and record the finding. This evaluation is done every 15 minutes or more often, depending on the patient’s conditions. • Airway • Vital signs • Color • Skin • Level of consciousness • Fluid and electrolyte balance • Dressings, tubes, drains, or casts • Position • Safety measure • Physician’s orders • Comfort of the patient • Reporting and Recording
PACU POSTOPERATIVE COMPLICATION • Circulatory problems - Shock - Hemorrhage - Femoral phlebitis or thrombosis • Pulmonary complications - Atelectasis • Urinary complications - Urinary retention - Urinary incontinence
Perioperative Nursing • How to describe an operation - the terminology used to describe all operations is a composite of basic Latin or Greek . - describe the organ to be operated on lapar-, abdomen (laparus = flank);
nephro-, kidney pyelo-, renal pelvis cysto-, bladder chole-, bile/the biliary system col(on)-, large bowel hystero-, uterus thoraco-, chest rhino-, nose masto/mammo-, breast
Perioperative Nursing • describe any other organs or things involved in the procedure docho-, duct angio-, vessel (blood- or bile-carrying) litho-, stone • describe what is to be done -otomy, to cut (open) -ectomy, to remove -plasty, to change shape or size -pexy, to change position -raphy, to sew together -oscopy, to look into -ostomy, to create an opening in (stoma = mouth) -paxy, to crush -graphy/gram, image (of)
Perioperative Nursing • Add any to qualify how or where the procedure is done percutaneous, via the skin; trans-, across; antegrade, forward; retrograde, backwards.
• Choledochoduodenostomy: an opening between the bile duct and the duodenum • Rhinoplasty: nose reshaping • Bilateral mastopexy: breast lifts • Percutaneous arteriogram: arterial tree imaging by direct puncture injection • Loop ileostomy: external opening in the small bowel with two sides • Flexible cystourethroscopy: internal bladder and urethral inspection
Venus Sofia J. Balatero, RN, USRN
Perioperative Nursing • Perioperative nursing is not just "technical work anyone can do". Perioperative nurses are skilled, knowledgeable RNs that care for patients before, during, and after surgery. • The fundamental nursing values (knowledge, skills, and judgment) are ever present and are the basis of the quality of care that surgical patients have relied on and can expect.
Perioperative Nursing
•The patient is the center of the sterile field
Perioperative Nursing The OR team usually consists of: • Surgeon: Scrubbed and in surgical attire to perform the surgery • Anesthesia provider: Masked and in clean scrub attire to ister the anesthesia - During the procedure the anesthesiologist monitors the patient’s vital signs and is responsible for keeping the surgeon aware of the patient’s condition. The anesthesiologist determines when the patient may be moved to the post anesthesia recovery stretcher after the surgical procedure has been completed. This person usually checks the patient’s airway and vital signs before taking the patient to the post anesthesia recovery room.
Perioperative Nursing The OR team usually consists of: • Surgical assistant (first assistant):
Can be another physician, a nurse, or physician’s assistant (PA) who is scrubbed, in sterile attire, and assists the surgeon to ligate, suction, and suture • Scrub nurse: Scrubbed and in sterile attire; prepares the instrument tray and es the instruments, sponges, needles, and sutures to the surgeon • Circulating nurse: In clean scrub attire and mask; assure that sterility is maintained at all times; obtains supplies, delivers materials, pours solutions, handles specimens, positions the client and surgical drapes, and disposes of soiled items
Perioperative Nursing
• PHASES –Perioperative –Intraoperative –Postoperative
Perioperative Nursing • PREOPERATIVE PHASE – Begins when the decision is made to undergo surgical intervention and it ends when the patient is transferred to the OR bed – During this phase, the perioperative nurse performs the assessment, determines the nursing diagnoses, identifies potential outcomes and develops a plan of care – The perioperative nurse plans, prioritizes, and initiates the patient care necessary for the attainment of the desired outcomes
Perioperative Nursing • INTRAOPERATIVE PHASE -Begins with the placement of the patient on the OR bed and continues until the patient is itted to a postprocedure or postoperative area -Implementation of the plan and evaluation of care continues during this phase.
Perioperative Nursing • POSTOPERATIVE PHASE -Begins with ission of the patient to a postprocedure or postanethesia area, which may be a postanesthesia care unit (PACU) or an intensive care unit (ICU). -Patients itted to the facility on an ambulatory 1-day-stay basis may return to the ambulatory unit. As indicated by his condition, the patient will transfer from the immediate postoperative patient care division for progressive stages of self-care on a surgical unit before being discharged from the hospital. -The postoperative phase ends when the surgeon discontinues follow-up care -Evaluation, the sixth component of the nursing process, is completed during this phase
Perioperative Nursing Phase Preoperative
From
To
Decision for surgical Transfer to intervention Operating Room
Intraoperative Received in Operating Room
ission to Recovery Room
Postoperative ission to recovery Room
Follow-up Evaluation
Type of Surgery acc. to URGENCY Type of Surgery
Optional Elective Planned/ Required Urgent/ Imperative Emergency
Time requirement for surgery At the preference of patient; surgery not needed At the convenience of patient as failure to have surgery is not catastrophic Within a few weeks as surgery is important Within 24-48 hours
Example Cosmetic surgery Liposuction Excision of superficial cyst Cataract extraction Cancer surgery
Immediately without delay to Intestinal maintain life or organ, Obstruction remove damage, stop bleeding
Type of Surgery acc. to PURPOSE Type of Surgery
Diagnostic Exploratory
Purpose
Example
To confirm diagnosis
Excision and biopsy To estimate the extent of the Exploratory disease and confirm Laparotomy diagnosis as well
Curative -Ablative Removal of diseased organ -Constructive Repair of congenital defects -Reconstructive Restoration of damaged organ Palliative Relieves symptom but does not cure the disease
Hysterectomy Repair of cleft lip or palate Episiorrhapy Rhizotomy and chordotomy (for pain relief)
Type of Surgery acc. to SERIOUSNESS Type of Surgery
Minor Major
Extent of Surgery Surgery that involves minimal (few) complications and minimal blood loss Extensive surgery that involves serious risk and complications (and loss of blood) as it involves major organs
Sterile Technique
Sterile Technique • Strict adherence to sound principles of sterile technique and recommended practices is mandatory for the safety of the patient. • This adherence reflects one’s surgical conscience. • Principles remain the same; it is the degree of adherence to them that varies.
Principles of Sterile Technique • Sterile persons have scrubbed and are gowned and gloved; unsterile person have not. • Only Sterile Items Are Used Within the Sterile Field. • If you are in doubt about the sterility of anything, consider it not sterile. • Gowns Are Considered Sterile Only from the Waist to Shoulder Level Front and the Sleeves • Tables Are Sterile Only at Table Level
Principles of Sterile Technique • Persons Who Are Sterile Touch Only Sterile Items of Areas; Persons Who Are Not Sterile Touch Only Unsterile Items or Areas • Unsterile Persons Avoid Reaching over a Sterile Field; Person Avoid Leaning over an Unsterile Area • Edges of anything that encloses Sterile Contents are Considered Unsterile • Sterile Field is Created as close as Possible to time of Use
Principles of Sterile Technique • Sterile Areas are Continuously Kept in View • Sterile Persons Keep well within the Sterile Area - They do not walk around or go outside room - Sterile Persons keep wit Sterile Areas to a Minimum • Unsterile Persons Avoid Sterile Areas • Destruction of Integrity of Microbial Barriers Results in Contamination - Strike-through is soaking of moisture through unsterile layers to sterile layers or vice-versa. • Microorganism Must be kept to an Inducible Minimum
Perioperative Nursing • PATIENTS SKIN PREP - done after patient has been anesthetized and positioned on the operating table, skin of the operative site and extensive area surrounding it is mechanically cleansed again with an antiseptic agent immediately prior to draping
Perioperative Nursing
• PATIENTS SKIN PREP - Responsibility: The first assistant is the person who scrubs the patient after he has scrubbed his own hands and arms
Perioperative Nursing • PATIENTS SKIN PREP - Scrub skin, starting at site if incision, with a circular motion or over widening circles to the periphery. Use enough pressure and friction to remove dirt and microorganisms from skin and pores. - Discard sponge after reaching periphery. Never bring a soiled sponge back toward center of area
Perioperative Nursing • Contaminated Areas within the Operative Field: - Umbilicus, stoma, draining sinuses, skin ulcer, vagina, anus, colostomy, (In all contaminated areas, follow general rule of scrubbing the most contaminated area last of with a separated sponge
Layers of Tissue The five main layers of abdominal tissue from the outer most are: • Skin • Subcutaneous • Fascia • Muscle • Peritoneum
PACU
PACU • The post anesthesia recovery room is rarely called an intensive care unite, but it is. • Everyday is a real challenge to PACU nurses because many kinds of situations occur. They are expected to have good knowledge of both medical and surgical procedures because they care for patients with all types of medical and surgical problems. The nurses must be calm and in full command of the situation but know their limitations • The PACU nurse works under the direction of the anesthesiologist or surgeon. The nurse must carry out simultaneously four assignments: - Observation of the patient - Evaluation of those observations - Performance of the necessary treatment - Reporting and recording observations and treatment • Total care of the patient requires both-in-depth study and experience in post anesthesia recovery nursing.
PACU • The PACU nurse must totally evaluate the patient and record the finding. This evaluation is done every 15 minutes or more often, depending on the patient’s conditions. • Airway • Vital signs • Color • Skin • Level of consciousness • Fluid and electrolyte balance • Dressings, tubes, drains, or casts • Position • Safety measure • Physician’s orders • Comfort of the patient • Reporting and Recording
PACU POSTOPERATIVE COMPLICATION • Circulatory problems - Shock - Hemorrhage - Femoral phlebitis or thrombosis • Pulmonary complications - Atelectasis • Urinary complications - Urinary retention - Urinary incontinence
Perioperative Nursing • How to describe an operation - the terminology used to describe all operations is a composite of basic Latin or Greek . - describe the organ to be operated on lapar-, abdomen (laparus = flank);
nephro-, kidney pyelo-, renal pelvis cysto-, bladder chole-, bile/the biliary system col(on)-, large bowel hystero-, uterus thoraco-, chest rhino-, nose masto/mammo-, breast
Perioperative Nursing • describe any other organs or things involved in the procedure docho-, duct angio-, vessel (blood- or bile-carrying) litho-, stone • describe what is to be done -otomy, to cut (open) -ectomy, to remove -plasty, to change shape or size -pexy, to change position -raphy, to sew together -oscopy, to look into -ostomy, to create an opening in (stoma = mouth) -paxy, to crush -graphy/gram, image (of)
Perioperative Nursing • Add any to qualify how or where the procedure is done percutaneous, via the skin; trans-, across; antegrade, forward; retrograde, backwards.
• Choledochoduodenostomy: an opening between the bile duct and the duodenum • Rhinoplasty: nose reshaping • Bilateral mastopexy: breast lifts • Percutaneous arteriogram: arterial tree imaging by direct puncture injection • Loop ileostomy: external opening in the small bowel with two sides • Flexible cystourethroscopy: internal bladder and urethral inspection
Related Documents c2h70
Operating Room Techniques md2q
October 2019 47
Operating Room Orientation Manual 421w15
October 2019 70
Operating Room Drugs t692e
November 2021 0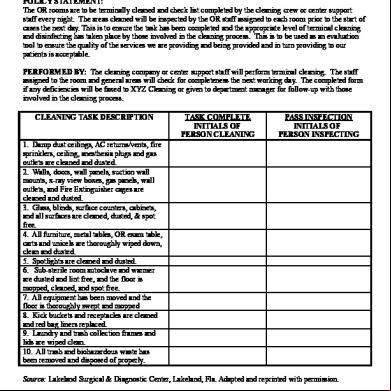
Operating Room Cleaning Checklist q1f4p
November 2019 175
Operating Room Charting 5cpl
November 2021 0
Operating Room Basic Instruments 5n63m
December 2019 48More Documents from "Rou Kun Ye" 1u2h4w
Operating Room Techniques md2q
October 2019 47
Life Is Elsewhere - Milan Kundera.pdf 6r4a72
October 2019 46
Terminal Evacuation Plan 1l2x1c
January 2022 0
Createspace.elements.of.programming.interviews.in.java.the.insiders.guide.2nd.edition.1517435803.pdf 6c4n73
November 2019 231
Lirik Lagu Bendera Merah Putih 29u5i
November 2019 117