N Peptic Ulcer Ds b5sg
This document was ed by and they confirmed that they have the permission to share it. If you are author or own the copyright of this book, please report to us by using this report form. Report 2z6p3t
Overview 5o1f4z
& View N Peptic Ulcer Ds as PDF for free.
More details 6z3438
- Words: 454
- Pages: 4
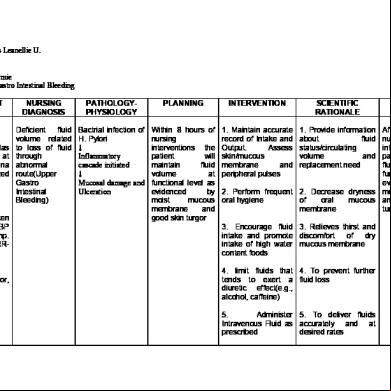
Guerrero, Precious Leanellie U. N3-7 Grp. 26 Patient: Abad, Hermie Problem: Upper Gastro Intestinal Bleeding ASSESSMENT Subjective: "Medyo madalas ako mauhaw at medyo nanghihina ako" as verbalized by the patient Objective: -Vital signs taken as follows: BP 130/90 Temp. 36.2oc CR- 64 RR20 -pallor -body weakness Poor skin turgor, dry skin -dry mouth
NURSING DIAGNOSIS
PATHOLOGYPHYSIOLOGY
PLANNING
INTERVENTION
SCIENTIFIC RATIONALE
Deficient fluid volume related to loss of fluid through abnormal route(Upper Gastro Intestinal Bleeding)
Bactrial infection of H. Pylori ↓ Inflammatory cascade initiated ↓ Mucosal damage and Ulceration
Within 8 hours of nursing interventions the patient will maintain fluid volume at functional level as evidenced by moist mucous membrane and good skin turgor
1. Maintain accurate record of Intake and Output. Assess skin/mucous membrane and peripheral pulses
1. Provide information about fluid status/circulating volume and replacement need
EVALUATION
After 8 hours of nursing interventios the patient maintained fluid volume at functional level as evidenced by moist 2. Perform frequent 2. Decrease dryness mucous membrane oral hygiene of oral mucous and good skin membrane turgor 3. Encourage fluid 3. Relieves thirst and intake and promote discomfort of dry intake of high water mucous membrane content foods 4. limit fluids that 4. To prevent further tends to exert a fluid loss diuretic effect(e.g., alcohol, caffeine) 5. ister 5. To deliver fluids Intravenous Fluid as accurately and at prescribed desired rates
Guerrero, Precious Leanellie U. N3-7 Grp. 26 Patient: Abad, Hermie Problem: Anxiety
ASSESSMENT Subjective:
NURSING DIAGNOSIS
Anxiety related to threat to/ or "hindi ko alam change in kung health status makakapagtrabaho na ako kaagad pagkagaling ko eh" as verbalized by the patient Objective: - Vital signs taken as follows: BP 130/90 Temp. 36.2oc CR- 64 RR20 -restlessness -difficulty in sleeping -fatigue
PLANNING
INTERVENTION
SCIENTIFIC RATIONALE
Within 8 hours of nursing interventions the patient will appear relaxed and the level of anxiety will reduced to a manageable level
1. Monitor vital signs(e.g., rapid or irregular pulse, rapid breathing)
1. To identify physical responses associated with both medical and emotional conditions
2. Use presence, touch, verbalization or demeanor to remind client and to encourage expressions or clarification of needs, concerns, unknowns and questions
EVALUATION
After 8 hours of nursing interventios the patient appeared relaxed and the 2. Being ive level of anxiety will and approachable reduced to a encourages manageable level communication
3. Accept client's defenses, do not confront, argue and debate
3. If defenses are not threatened, the client may feel safe enough to look at the behavior
4. Allow and reinforce clients personal reaction towards the threatens to well being
4. Talking or otherwise expressing feeling reduces anxiety
5. Explain everything necessary regarding the disease
5. To educate the patient regarding the disease to reduce anxiety
NURSING DIAGNOSIS
PATHOLOGYPHYSIOLOGY
PLANNING
INTERVENTION
SCIENTIFIC RATIONALE
Deficient fluid volume related to loss of fluid through abnormal route(Upper Gastro Intestinal Bleeding)
Bactrial infection of H. Pylori ↓ Inflammatory cascade initiated ↓ Mucosal damage and Ulceration
Within 8 hours of nursing interventions the patient will maintain fluid volume at functional level as evidenced by moist mucous membrane and good skin turgor
1. Maintain accurate record of Intake and Output. Assess skin/mucous membrane and peripheral pulses
1. Provide information about fluid status/circulating volume and replacement need
EVALUATION
After 8 hours of nursing interventios the patient maintained fluid volume at functional level as evidenced by moist 2. Perform frequent 2. Decrease dryness mucous membrane oral hygiene of oral mucous and good skin membrane turgor 3. Encourage fluid 3. Relieves thirst and intake and promote discomfort of dry intake of high water mucous membrane content foods 4. limit fluids that 4. To prevent further tends to exert a fluid loss diuretic effect(e.g., alcohol, caffeine) 5. ister 5. To deliver fluids Intravenous Fluid as accurately and at prescribed desired rates
Guerrero, Precious Leanellie U. N3-7 Grp. 26 Patient: Abad, Hermie Problem: Anxiety
ASSESSMENT Subjective:
NURSING DIAGNOSIS
Anxiety related to threat to/ or "hindi ko alam change in kung health status makakapagtrabaho na ako kaagad pagkagaling ko eh" as verbalized by the patient Objective: - Vital signs taken as follows: BP 130/90 Temp. 36.2oc CR- 64 RR20 -restlessness -difficulty in sleeping -fatigue
PLANNING
INTERVENTION
SCIENTIFIC RATIONALE
Within 8 hours of nursing interventions the patient will appear relaxed and the level of anxiety will reduced to a manageable level
1. Monitor vital signs(e.g., rapid or irregular pulse, rapid breathing)
1. To identify physical responses associated with both medical and emotional conditions
2. Use presence, touch, verbalization or demeanor to remind client and to encourage expressions or clarification of needs, concerns, unknowns and questions
EVALUATION
After 8 hours of nursing interventios the patient appeared relaxed and the 2. Being ive level of anxiety will and approachable reduced to a encourages manageable level communication
3. Accept client's defenses, do not confront, argue and debate
3. If defenses are not threatened, the client may feel safe enough to look at the behavior
4. Allow and reinforce clients personal reaction towards the threatens to well being
4. Talking or otherwise expressing feeling reduces anxiety
5. Explain everything necessary regarding the disease
5. To educate the patient regarding the disease to reduce anxiety
Related Documents c2h70
N Peptic Ulcer Ds b5sg
November 2019 107
Peptic Ulcer 5x7272
November 2020 0
Nursing Care Plan For Peptic Ulcer N nv4j
November 2019 474
Peptic Ulcer Disease 4531w
December 2019 35
Pathophysiology Of Peptic Ulcer 1n4q36
December 2019 201