Medical Charges Reimbursement Form 6d5c2s
This document was ed by and they confirmed that they have the permission to share it. If you are author or own the copyright of this book, please report to us by using this report form. Report 2z6p3t
Overview 5o1f4z
& View Medical Charges Reimbursement Form as PDF for free.
More details 6z3438
- Words: 376
- Pages: 3
H.P.T.R.6
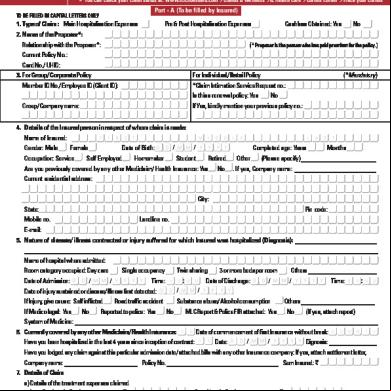
Medical Charges Reimbursement Form 1. Name and Designation
:
SUNDER LAL, Cook Retd.
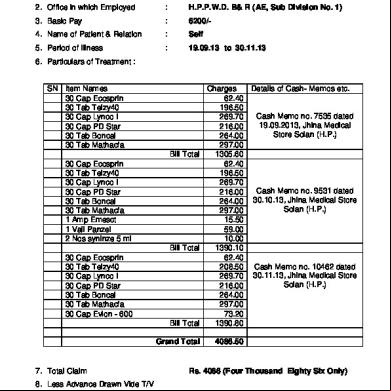
2. Office in which Employed
:
H.P.P.W.D. B& R (AE, Sub Division No. 1)
3. Basic Pay
:
6200/-
4. Name of Patient & Relation
:
Self
5. Period of Illness
:
19.09.13 to 30.11.13
6. Particulars of Treatment :
SN Item Names 30 Cap Ecosprin 30 Tab Telzy40 30 Cap Lynco I 30 Cap PD Star 30 Tab Boncal 30 Tab Mathacfa 30 Cap Ecosprin 30 Tab Telzy40 30 Cap Lynco I 30 Cap PD Star 30 Tab Boncal 30 Tab Mathacfa 1 Amp Emesct 1 Vail Panzel 2 Nos syninze 5 ml 30 Cap Ecosprin 30 Tab Telzy40 30 Cap Lynco I 30 Cap PD Star 30 Tab Boncal 30 Tab Mathacfa 30 Cap Evion - 600
Charges Details of Cash- Memos etc. 62.40 196.50 Cash Memo no. 7535 dated 269.70 19.09.2013, Jhina Medical 216.00 Store Solan (H.P.) 264.00 297.00 Bill Total 1305.60 62.40 196.50 269.70 Cash Memo no. 9531 dated 216.00 30.10.13, Jhina Medical Store 264.00 Solan (H.P.) 297.00 15.50 59.00 10.00 Bill Total 1390.10 62.40 208.50 Cash Memo no. 10462 dated 269.70 30.11.13, Jhina Medical Store Solan (H.P.) 216.00 264.00 297.00 73.20 Bill Total 1390.80 Grand Total
7. Total Claim
4086.50
Rs. 4086 (Four Thousand Eighty Six Only)
8. Less Advance Drawn Vide T/V No. _________ Drt._______ 9. Net amount payable
Rs. Rs. 4086 (Four Thousand Eighty Six Only)
I hereby declare that the statements in this application are true to the best of my knowledge and belief and that the person for whom medical expenses were incurred is wholly dependent on me.
Date
(Signature of claimant)
VERIFICATION CERTIFICATE I Dr. __________________________ hereby certify that ______________________ Suffering from _________________________________ and is / was under my treatment From _________________ to _________________ and that the above mentioned medicines /tests were prescribed by me in this connection. The claim is verified for Rs. ____________________
Date :_______________________
(Signature of Medical Officer) Designation & Seal
-----------------------------------------------------------------------------------------------------------------------------ed for Rs. ________________________ (Rupees )__________________________ _____________________ and included in Bill no. ________________ Dated ______________
(Signature of controlling Officer)
(Signature of the DDO)
--------------------------------------------------------------------------------------------------------------------------Instructions 1. List all the medicines, tests etc. individually 2. Attach Cash-Memos duly verified. 3. Mention dates of ission to the Hospital, stay etc.
-
Medical Charges Reimbursement Form 1. Name and Designation
:
SUNDER LAL, Cook Retd.
2. Office in which Employed
:
H.P.P.W.D. B& R (AE, Sub Division No. 1)
3. Basic Pay
:
6200/-
4. Name of Patient & Relation
:
Self
5. Period of Illness
:
19.09.13 to 30.11.13
6. Particulars of Treatment :
SN Item Names 30 Cap Ecosprin 30 Tab Telzy40 30 Cap Lynco I 30 Cap PD Star 30 Tab Boncal 30 Tab Mathacfa 30 Cap Ecosprin 30 Tab Telzy40 30 Cap Lynco I 30 Cap PD Star 30 Tab Boncal 30 Tab Mathacfa 1 Amp Emesct 1 Vail Panzel 2 Nos syninze 5 ml 30 Cap Ecosprin 30 Tab Telzy40 30 Cap Lynco I 30 Cap PD Star 30 Tab Boncal 30 Tab Mathacfa 30 Cap Evion - 600
Charges Details of Cash- Memos etc. 62.40 196.50 Cash Memo no. 7535 dated 269.70 19.09.2013, Jhina Medical 216.00 Store Solan (H.P.) 264.00 297.00 Bill Total 1305.60 62.40 196.50 269.70 Cash Memo no. 9531 dated 216.00 30.10.13, Jhina Medical Store 264.00 Solan (H.P.) 297.00 15.50 59.00 10.00 Bill Total 1390.10 62.40 208.50 Cash Memo no. 10462 dated 269.70 30.11.13, Jhina Medical Store Solan (H.P.) 216.00 264.00 297.00 73.20 Bill Total 1390.80 Grand Total
7. Total Claim
4086.50
Rs. 4086 (Four Thousand Eighty Six Only)
8. Less Advance Drawn Vide T/V No. _________ Drt._______ 9. Net amount payable
Rs. Rs. 4086 (Four Thousand Eighty Six Only)
I hereby declare that the statements in this application are true to the best of my knowledge and belief and that the person for whom medical expenses were incurred is wholly dependent on me.
Date
(Signature of claimant)
VERIFICATION CERTIFICATE I Dr. __________________________ hereby certify that ______________________ Suffering from _________________________________ and is / was under my treatment From _________________ to _________________ and that the above mentioned medicines /tests were prescribed by me in this connection. The claim is verified for Rs. ____________________
Date :_______________________
(Signature of Medical Officer) Designation & Seal
-----------------------------------------------------------------------------------------------------------------------------ed for Rs. ________________________ (Rupees )__________________________ _____________________ and included in Bill no. ________________ Dated ______________
(Signature of controlling Officer)
(Signature of the DDO)
--------------------------------------------------------------------------------------------------------------------------Instructions 1. List all the medicines, tests etc. individually 2. Attach Cash-Memos duly verified. 3. Mention dates of ission to the Hospital, stay etc.
-
Related Documents c2h70
Medical Charges Reimbursement Form 6d5c2s
October 2021 0
Medical Claim Reimbursement Form English 6q276v
November 2019 163
Medical Reimbursement Information 5j304y
September 2020 0
Medical Reimbursement Covering Letter 326f1u
October 2019 79
Claim Form Dhs Reimbursement 5s4j4m
October 2019 73