Liver Cirrhosis Case Presentation 4r423w
This document was ed by and they confirmed that they have the permission to share it. If you are author or own the copyright of this book, please report to us by using this report form. Report 2z6p3t
Overview 5o1f4z
& View Liver Cirrhosis Case Presentation as PDF for free.
More details 6z3438
- Words: 19,758
- Pages: 146
ACKNOWLEDGEMENT
The group would like to express their heartfelt gratitude, sincere appreciation and profound regards to the following people who, in one way or another, gave guidance, strength, and encouragement in making this case presentation possible. First of all, to Almighty God the Father, who granted us the knowledge and skills, Who send forth the gift of Holy spirit that aided them in completing this study. Without Him, none of these things would be possible. To their family, friends, and classmates, for their consideration and unending , emotionally, spiritually and financially. To their clinical instructor, Mrs. Jocelyn Ferraren, RN, for guiding us in the course of making this case presentation and giving them tips on how to have a good presentation. To all medical personnel and staff of DMC, MED- ward, for the warm accommodation during their clinical exposure and for giving them inspiration to keep the spirit of caring burning. To the of the group, for sharing ideas, cooperating and giving full effort in making the case presentation successful.
1
Lastly, to our client and his family for their acceptance and willingness to share time, effort and giving us the essential information needed for this case presentation.
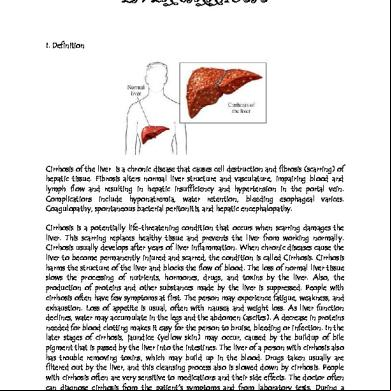
INTRODUCTION The liver is one of the largest and most complex organs in the body. It stores vital energy and nutrients, manufactures proteins and enzymes necessary for good health, protects the body from disease, and breaks down (or metabolizes) and helps remove harmful toxins, like alcohol, from the body. It is one of the most important organs in the body since it has many significant functions. A lack or failure to provide proper care of it may lead to an abnormality or disorder. One of the severe forms that may happen is Liver Cirrhosis. Liver Cirrhosis is derived from Greek word kirrhos, meaning "tawny" (the orange-yellow colour of the diseased liver).It is a chronic disease that causes cell destruction and fibrosis (scarring) of hepatic tissue. Fibrosis alters normal liver structure and vasculature, impairing blood and lymph flow and resulting in hepatic insufficiency and hypertension in the portal vein. Cirrhosis is most commonly caused by alcoholism, hepatitis B and C and fatty liver disease but has many other possible causes. Some cases are idiopathic, i.e., of unknown cause. It may be classified by the structural changes that take place or by the cause of the disorder. Internationally, liver cirrhosis is the 8thth most common cause of death. It is most common among people ages 45 – 75, killing more than 25,000 people each year, 50% of which are alcohol related. In the Philippines and other underdeveloped countries,
2
however, the incidence of liver cancer is rather high. Liver cancer is relatively common in our country primarily because many Filipinos suffer from cirrhosis of the liver, a major risk factor for liver cancer. Cirrhosis of the liver precedes 80 percent of all liver cancers; thus, any condition that predisposes to cirrhosis indirectly causes liver cancer. The usual cause of liver cirrhosis among Filipinos is chronic hepatitis B, a major public health problem in the country. Chronic hepatitis B afflicts between 10 and 12 percent of all Filipinos (i.e., more than 8 million Filipinos). Other less significant causes of cirrhosis are hepatitis C infection and alcoholism. The latest DOH advisory shows that liver cancer is the third most common form of cancer among Filipinos—in men, it is the second most common, while in women, it is the ninth most common. Locally, liver cirrhosis is the 17th leading cause of death here in Davao. In connection with it, last February 11, 2010, the Group 3 of section 3H was assigned on duty at the Davao Medical Center- Communicable Pavilion where they met their patient Mr. Cute who was diagnosed of having Liver Cirrhosis. They were motivated to learn more and study the disorder since it was their first time to encounter such case. Also, the group was more encouraged to choose the patient for their case presentation in order to acquire better understanding and to gain more knowledge and use it for the future.
3
OBJECTIVES To have a course of direction, organization and to recognize the essence of this study, we have set the following objectives:
GENERAL OBJECTIVES
After rendering effective nursing care for three days at the Davao Medical Center, MED- Ward, we aim: • To provide an extensive study about Community acquired pneumonia ascites
secondary to liver cirrhosis for us to gain better understanding about the disease and be equipped with competence in dealing with related situations in the future; • To improve our skills in doing relevant interventions which promote wellness to
persons having the disease; •
Not only to understand the situation of the client and their families who are confronted with the disease but also to empathize with them.
SPECIFIC OBJECTIVES
Find a case in the DMC, MED- ward within the three-day duty;
4
Establish a good interpersonal relationship with our chosen client as well as to his significant others;
Acquire necessary data of our client which are relevant to our case study;
Trace the patient’s family lineage and present remarkable familial disease;
Trace the health history of the client and the family by collecting information both from the past and present illnesses;
Evaluate the client’s development guided by Erik Erikson, Robert Havighurst and Jean Piaget’s Theory;
Define the complete diagnosis of our client guided by three different sources;
Perform cephalocaudal assessment to the client thoroughly;
Discuss the systems involved in the development of the disease in the human anatomy and physiology;
Present the etiology and symptomatology of the disease process with each of its rationales and identify which are present on the client’s case;
Trace the pathophysiology of the disease as experienced by our client and
Sends thesignal to the medulla oblongata to presentcough Crackles and Wheezes
it through a schematic diagram;
Present and analyze the doctor’s order in chronological manner;
Explain and interpret both actual and possible diagnostic studies including indication, result, and their implications;
The mucosal lining nerves detects the excessive the secretions
Exudates production and Edema Cilia try to propels the mucous out of the 5 system Stimulates mucous
large quantities
Discuss the different drugs taken by the patient with corresponding intervention;
Identify different nursing theories made by
Florence Nightingale,
Chemical mediators irritate the goblet cells of the bronchial nursing lining Stimulates Diapedesis and positive Virginia chemotaxis of Leukocytes
Henderson and Lydia Hall and relate it on the patient’s conditions;
Inflammation of the Parenchyma
Formulate specific, measurable, attainable, realistic, and time-bounded nursing care plans with corresponding rationales for each of the nursing interventions;
Evaluate the client’s progress with our continuous care; Render health teachings or appropriate nursing interventions necessary client and family as well;
Present a discharge plan for the patient
Fever
Obstruction of the airway
Cilia fail to sweep the mucous to the because of thickness Histamine causes vasodilation Prostaglandin and Leukotrienes causes blood vessels to be more permeable
Present and justify the prognosis of our patient
Provide recommendations for the better management of patient with the same disease in the future endeavor;
Accomplish our case presentation.
Damage of the cells release Histamine, Prostaglandins and Leukotrienes Blood vessels leak. Damage on the blood vessels is scant Predisposing factors: Age- elderly adults (age above 70)
Precipitating factors: Smoking Alcoholism
6 Hematemesis and
GI bleeding If treated: MGT: Transplantatio n Paracentesis Medications
PATIENT’S DATA
Name: Mr. Cutie Age: 72 years old Sex: Male Date of birth: May 23, 1937 Place of birth: Igacos, Davao City Current address: Manablay Callawa, Buhangin Davao City Occupation: Farmer Nationality: Filipino Religion: Christianity (Roman Catholic) Civil Status: Married
plasmaphorese s If not treated Progressive liver destruction, systemic counsel Hepatic encephalopath y Toxic substance production Mental retardation Hepatic coma
DEATH
Date of ission: February 6, 2010
- Destruction of cell membranes causes red blood cells to burst
Time of ission: 04:09PM
Nursing Resp:
CLINICAL DATA
Mode of ission: Ambulatory Chief complaint: malaise, loss of appetite, nausea, and black tarry stool
-Give supplements containing Vit.E
Nursing Resp: 7 -Give Vit.D fortified milk
-Give supplementati on
Ward: MED - itting physician: Dr. Emerson R. Taghoy Vital signs upon ission: Temp: 36.6 C BP: 90/60 mmHG PR: 65 bpm RR: 28 m Final diagnosis: CAP MR Ascites 2’ Liver Cirrhosis Source: Significant others and patient's chart
Varices and hemorrhoids May rupture and bleed Vitamin D Decrease absorption of calcium and Phosphorus from the GI tract Vitamin E Decrease against oxidative damage caused by free radicals Nursing Resp:
- Monitor urine output - Elevate edematous extremities -Reposition every 2 hours if patient - ister diuretics as prescribed - Tell patient to use antiembolic stockings or bandage 8 Nursing Resp: -Give
-prevent injury -decrease risk for infection
Development of tissues, and resistance to infections
GENOGRAM Lola-har
Lolo-har
Grandmade r
Body malaise
Titahar
PAPA-HAR
Manong
Decreased source of MAMA-HARenergy Auntie Decreased glucose in the body
Tito
Kol
Decreased vitamin K Gwaping
Boylet
Gwafa
Keks
Pefa A Vitamin
Cutie●
Vitamin deficiency Nursing Resp: -Encourage intake of Vit.K rich foods
LEGEND: MALE FEMALE
DECEASED TB HYPERTENSION ●
LIVER CIRRHOSIS
Nursing Resp: Nursing Resp: -Assess pain scale -Monitor VS -ister analgesic as ordered
9
Absence of bilirubin in the feces
FAMILY BACKGROUND AND HEALTH HISTORY Family History
Bile unable to reach Gi tract Clay colored stool ASCITES
Most of the significant details gathered on the interview we had came from
Third spacing occurs Mr.Cutie’s wife and daughter since he was not able to verbalize due to his condition. JAUNDICE
Upon the interview, we found out that no one in the family had any of the sickness that the patient had namely Liver Cirrhosis and Community Acquired Pneumonia.
Speeds up destruction of RBCs
Cutie is a married man with three children. He is the main decision maker in the
Chronic ive family as evidenced by his wife verbalizing,” siya man gyud ng gabuot ug unsay maayo congestion
para sa amoa”. In regards to their health, several of their family specifically the Spleen patient, his wife and his daughter have hypertension which was all diagnosed by GI the tract physician, whom they usually consult in Polyclinic Health Center where their neighbor Stomach pain works as a nurse. However they were not able to recall the name of the physicianAltered they bowel function
consulted, but they were able to the month and year that their condition was
Blood regurgitation diagnosed: on August of the year 2009. In reference to the diagnosis that was given by to the spleen , tract the physician, maintenance medication was given to the three of them howeverGIthey Prominent forgot since they only used the said the medication for about two weeks. Finances were a
distended factor since they were not able to comply the medication prescribed by the physician.blood vessels in the stomach Bleeding The family does not seek medical advice until the condition they have worsens as tendencies
stated by Cutie’s wife. All of them had experienced fever, flu, cough, colds, stomach
Shunting of pains, etc. but again they don’t seek medical attention until condition becomes worse.blood from portal vessels to vessels with lower pressure Decrease in osmotic pressure 10 KIDNEYS
Signal for aldosterone release
Lifestyle
Na+ absorption/ H2O retention
As verbalized by the patient’s wife, the patient at his young age was a typicalK+ excretion
adolescent who goes with friends and often explores things around. As stated, the patient
EDEMA
was curious at all things and because of that he was inclined to a number of vices which
No free blood age may actually have affected his health status. He was smoking badly as he was able to Backflow of bile
consume 1-2 packs of cigarette a day and drinks enormously as he was able to drink 1
long neck of Tanduay on his own. At times, he goes beyond 1 long neck and even drinks Bile goes to the blood
half a gallon of “Tuba” when he is not yet drunk. As stated by his wife, his husband doesstream
not stop drinking unless he becomes drunk. As the normal things go as stated by his Formation of collateral
wife, the patient and his drinking colleagues use same glass whenever they drink. All of vessels blood these had been the lifestyle of the client since then.
in the GI system Accumulation of ammonia
When he reached his adulthood, he worked as a farmer and still continued to
drink and smoke whenever he has time. He often sleeps at 10:00pm and wakes Unable up at to convert ammonia to urea
5:00am then takes his breakfast and goes to his work. He takes his break from 11:30am up to 12:30pm and thus eats his lunch. He goes to work and ends at 5:00pm. What he
Decreased
normally does is clean the plantation and get rid of unwanted growth of grasses allglucogenesis over the place that may alter the good growth of the trees that were present. Whenever he has Decrease in albumin
spare time such as weekends which is his rest day from work, he stays at home, watches production TV or talks with his children or goes to his neighbor and drinks. He had such routine Obstruction until of portal
last year, 2009, when he finally had stopped doing his usual things when he was circulation diagnosed of having hypertension. He drinks rarely and smokes only about 2-4 sticks aPortal day compared before when he was not yet diagnosed with hypertension.
hypertension Liver Decreased RBC 11 Body malaise, pallor
Change to Fowler’s position, assess CRT
Decreased erythropoietin
Diet
Hepatic fibrosis
The patient’s wife was able to notice that his husband was fond of eating fatty Impaired hepatocyte
foods such as “taba sa baboy.” Whenever they have this kind of viand, she reported that function
her husband would really eat a lot of these when available. She also mentioned that her changes Matrix husband liked eating salty foods such as dried fish and ginamos almost every day. It Extracellular has matrix
been said by the patient’s wife that these viands are the usual part of every meal.components In Predisposing addition to that, they often take canned goods. As the patient’s wife verbalized “Syempre Factors:
dong ana man gyud na sa pobre”. Moreover, drinking coffee every morning has always Male
been the routine of his husband, still reported by his wife.
Age (45-75 yrs old) Race
History of past illness Race: Asian
Other than ordinary fever, cough, and flu, which they treat only through over-thePathophysiology counter drugs and no consultations, the patient didn’t have any serious illness. This was of Liver Cirrhosis the case, however, until he reached the old age when different signs and symptoms started to manifest, increased blood pressure arise. He then sought medical advice since Precipitating factors:
there were other manifestations of hypertension such as dizziness, nausea and pain on his
nape. Then he found out that he has hypertension as diagnosed. Only through daily BP Chronic alcoholism
taking at Santo Tomas Clinic, a clinic just around the area, did they found out about this Diet
gradual increase in blood pressure. It was treated and taken cared of through unrecalled Smoking
medications that were prescribed to him by the said clinic. sMOK Portal obstruction Grandfader 12
History Of Present Illness For the past years, the patient did not have any serious illness related to his present condition. But on January 23, 2010, 2 weeks prior to the patient’s ission, he had headache, chest pain, dull abdominal pain, felt nauseated and dizzy. The patient and even his wife had never thought that it was a manifestation of an underlying problem and so they did not take it seriously. They did not seek medical attention; instead his wife gave him over-the-counter medication such as Paracetamol for his headache which he took four times during that day and one Diatabs for his stomach pain which is actually not appropriate since the medication itself was wrong and that the underlying condition was not taken into consideration. The condition however did not last long since it was relieved one day after it occurred. The patient and his wife were relieved and thought that it was just a “Panuhot and Kabuhi”. One week prior to patient’s ission to the hospital, his wife noticed that his husband had abdominal distention which she abruptly noticed as evidenced by her verbalization, “Dili man kaayo na siya dako ug tiyan sa una. Murag ning kalit ra man. Atong mga last week sa January ra pud nako nabantayan”. On the 2nd day of February, 2010, four days prior to ission to the hospital the patient sought consultation at the Emergency Room since the patient felt loss of appetite, stomach pain which radiated to the patient’s back and prandial vomiting. Despite the manifestations seen on the client, he was discharged and was requested to have an ultrasound of the abdomen. Aside from that, it was again diagnosed that he has hypertension so antihypertensive medications were prescribed. Days had gone and on the
13
6th of February 2010, the patient experienced body malaise, loss of appetite, nausea, and black tarry stool which were his chief complaint that resulted to his ission to Davao Medical Center.
14
DEVELOPMENTAL DATA
Erik Erikson’s Psychosocial Theory of Development Theory
Stage
Result and Justification
Erik Erikson, in his
Integrity versus Despair
The patient has fully
Psychosocial Theory of
(65 years old and above)
achieved integrity.
development, believed that
This stage focuses on
According to his wife,
personality develops in a
reflecting back on life.
Cutie is already contented
series of stages. Erikson's
Integrity means feeling at
with his life. His wife
theory proposes that life is a
peace with oneself and the
verbalized "Kamao ka
sequence of developmental
world. No regrets or
dong, miskan ana ra na
stages or levels of
recriminations. Despair
akong bana, wala gyud na
achievement. He described
and/or 'Disgust' represent the
siya nagmahay ug taman-
eight stages of development
opposite disposition: feelings
taman sa mga
and in each stage signals a
of wasted opportunities,
nangahitabo sa among
task that must be
regrets, wishing to be able to
kinabuhi. Simple ra nga
accomplished. Our progress
turn back the clock and have
panginabuhi ra ang
through each stage is in part
a second chance. Those who
among panginabuhi pero
determined by our success,
are unsuccessful during this
wala gyud na siya nag
or lack of success, in all the
phase will feel that their life
dahum na mudato.
previous stages. Erikson
has been wasted and will
Kontento na siya sa amo.
also believed that the more
experience many regrets. The Okay na sa iya kay
success an individual has at
individual will be left with
napadako niya ug maayo
each developmental stage,
feelings of bitterness and
among mga anak,
15
the healthier the personality
despair. Those who feel
makahikahos mi sa pang
of an individual is.
proud of their
adlaw-adlaw." Despite of
accomplishments will feel a
it, the patient was not able
sense of integrity.
to send his three children
Successfully completing this
in college. Moreover, the
phase means looking back
patient has been alcoholic
with few regrets and a
for almost 60 years and
general feeling of
been smoking since his
satisfaction. These
teenage years. These
individuals will attain
habits are wasted
wisdom, even when
opportunity and Mr. cutie
confronting death.
has not attained the wisdom since he was not able to decipher that his vices would affect his health in the long run.
16
Robert Havighurst’s Developmental Task Theory Theory
Stage
Result and Justification
Havighurst believes that in
Later Maturity (60 and
The patient has not fully
every developmental stage,
above)
achieved this stage since
certain tasks are needed to be accomplished for one’s progression. In his theory, he proposes that growth and
This stage in a person’s life is concerned with the achievement of the following
each associated with six to ten tasks to be learned. Havighurst identified Six
accomplished. He has his circle of friends whose age is almost same with
tasks:
development is occurring during six stages in life,
some tasks are not
his. They drink and play 1. Adjusting to decreasing physical strength and health. 2. Adjusting to
cards together. But according to his wife, he is not still used to his deteriorating strength. We
Major Stages in human life
retirement and
always wanted to work or
covering birth to old age.
reduced income.
at least to keep his self
Infancy & early childhood (Birth till 6 years old),
3. Adjusting to death of a spouse.
Middle childhood (6-13 years old), Adolescence (13-
busy, same as the thing he has been doing when he was still younger, but his
4. Establishing an
strength is limiting him
18 years old), Early
explicit affiliation
already. Therefore, he was
Adulthood (19-30 years
with one’s age group.
not able to adjust from his
old), Middle Age (3060years old), and Later
5. Meeting civic and social
physical limitation due to aging.
17
maturity (60 years old and over). From there, Havighurst recognized that each human has three
responsibilities. 6. Establishing satisfactory physical living arrangements.
sources for developmental tasks. They are: * Tasks that arise from physical maturation: Learning to walk, talk, control of bowel and urine, behaving in an acceptable manner to opposite sex, adjusting to menopause. * Tasks that arise from personal values: Choosing an occupation, figuring out ones philosophical outlook. * Tasks that have their source in the pressures of society: Learning to read, learning to be responsible citizen. A developmental
18
task is “a task which arises at or about a certain period in the life of an individual, successful achievement of which leads to his happiness and to success with later tasks, while failure leads to unhappiness in the individual, disapproval by society, and difficulty with later tasks”.
JEAN PIAGET’S THEORY OF COGNITIVE DEVELOPMENT Theory
Stage
Result and Justification 19
Jean Piaget proposed a sequence of cognitive development that emphasized the relationship between action and thought. Each phase in his theory is characterized by the ways in which the person interprets and uses the environment. The individual learns by
Formal Operations This stage is characterized by formal reasoning. It is in this stage that a person’s acquisition of the ability to think abstractly, reason logically and draw conclusions from the information available is measured.
The patient did not achieve this cognitive stage. The patient is a chronic alcohol drinker and a smoker. From that alone, he must have thought that this will have a bad effect on his health. He was not able to reason out logically and did not
interacting with the
able to see the bigger
environment through
picture that can be brought
assimilation,
about by his vices that
accommodation and
these will result to illness.
adaptation.
20
DEFINITION OF COMPLETE DIAGNOSIS CAP MR Ascites 2’ Liver Cirrhosis
Community-Acquired Pneumonia Community-acquired pneumonia (CAP) is one of the most common infectious diseases addressed by clinicians. CAP is an important cause of mortality and morbidity worldwide. CAP is usually acquired via inhalation or aspiration of pulmonary pathogenic organisms into a lung segment or lobe. Less commonly, CAP results from secondary bacteremia from a distant source, such as Escherichia coli urinary tract infection and/or bacteremia. CAP due to aspiration of oropharyngeal contents is the only form of CAP involving multiple pathogens. Source: Handbook of Medical-Surgical Nursing 3rd Edition by Springhouse, 2006
Community-Acquired Pneumonia Community-acquired pneumonia (CAP) is a disease in which individuals who have not recently been hospitalized develop an infection of the lungs (pneumonia). CAP is a common illness and can affect people of all ages. CAP often causes problems like difficulty in breathing, fever, chest pains, and a cough. CAP occurs because the areas of
21
the lung which absorb oxygen (alveoli) from the atmosphere become filled with fluid and cannot work effectively. Patients at moderate risk (class IV of the Pneumonia Severity Index) and high risk (class V) should be hospitalized, given their much higher rates of death and complications. In general, most such patients are elderly and have two or more additional poor prognostic factors, such as serious coexisting conditions, abnormal vital signs, and abnormal laboratory values. Source: Medical-Surgical Nursing: A Psychophysiologic Approach by Luckmann and Sorensen, 2003
Community-Acquired Pneumonia Patients with community-acquired pneumonia often present with cough, fever, chills, fatigue, dyspnea, rigors, and pleuritic chest pain. When a patient presents with suspected community-acquired pneumonia, the physician should first assess the need for hospitalization using a mortality prediction tool, such as the Pneumonia Severity Index, combined with clinical judgment. Pneumonia Severity Index
Patient Characteristics
Points
Demographics Male Female
Age (years) Age (years) – 10 22
Patient Characteristics
Points
Nursing home resident Comorbid illness
+ 10
Neoplastic disease Liver disease Congestive heart failure Cerebrovascular disease Renal disease Physical examination findings
+ 30 + 20 + 10 + 10 + 10
Altered mental status Respiratory rate >30 breaths per minute Systolic blood pressure < 90 mm Hg Temperature < 35°C (95°F) or >40°C (104°F) Pulse rate >125 beats per minute Laboratory and radiographic findings
+ 20 + 20 + 20 + 15 + 10
Arterial pH < 7.35 Blood urea nitrogen >64 mg per dL (22.85 mmol per L) Sodium < 130 mEq per L (130 mmol per L) Glucose >250 mg per dL (13.87 mmol per L) Hematocrit < 30 percent Partial pressure of arterial oxygen < 60 mm Hg or oxygen percent
+ 30 + 20 + 20 + 10 + 10 + 10
saturation < 90 percent Pleural effusion Total points:
+ 10 _______ Mortality % (No. of
Recommended site of
Point total
Risk
Risk class patients)
care
No
Low
I
0.1 (3,034)
Outpatient
predictors ≤ 70 71 to 90 91 to 130 >130
Low Low Moderate High
II III IV V
0.6 (5,778) 2.8 (6,790) 8.2 (13,104) 29.2 (9,333)
Outpatient Inpatient (briefly) Inpatient Inpatient
Source: Stephanie Wessel Reyburn, M.D., M.P.H., Mayo School Of Graduate Medical Education, Rochester, Minnesota - Http://Www.Aafp.Org/Afp/2006/0201/P442.Html Accessed On February 21, 2010
23
Ascites Ascites is an accumulation of serous fluid in the abdominal cavity. The fluid accumulates primarily because of low production of albumin by the failing liver. An insufficient amount of protein in the capillaries causes plasma to seep into the abdominal cavity. The accumulated fluid causes a markedly enlarged abdomen. The fluid may cause severe respiratory distress as a result of elevation of the diaphragm. Source: Understanding Medical Surgical Nursing by Williams and Hopper, 2007
Ascites Ascites is the accumulation of fluid (usually serous fluid which is a pale yellow and clear fluid) in the abdominal (peritoneal) cavity. The abdominal cavity is located below the chest cavity, separated from it by the diaphragm. Ascitic fluid can have many sources such as liver disease, cancers, congestive heart failure, or kidney failure. Source: Medical-Surgical Nursing: A Psychophysiologic Approach by Luckmann and Sorensen, 2003
Ascites
24
Ascites is diagnosed by inspection of the fluid-filled abdomen, percussion for dullness and tapping of massive ascites to produce fluid waves. When these signs are accompanied by other manifestations of disease associated with ascites, usually cirrhosis, identification of the problem is validated.
Source: Handbook of Medical-Surgical Nursing 3rd Edition by Springhouse, 2006
Liver Cirrhosis Liver cirrhosis is the final stage of many types of liver injury. The cirrhotic liver varies in appearance, but a nodular consistency with hands of fibrosis (scar tissue) is prominent. The cirrhosis patient frequently presents with problems such as ascites, gastrointestinal bleeding and encephalopathy. The disease often progresses quietly until such as emergency occurs. Hepatomegaly (enlarged liver), splenomegaly (enlarged spleen), vascular changes, or abnormal laboratory tests may be the first indicator in the patient who is
25
Source: Medical-Surgical Nursing: A Psychophysiologic Approach by Luckmann and Sorensen, 2003
Liver Cirrhosis A chronic hepatic disease, cirrhosis is characterized by diffuse destruction and fibrotic regeneration of hepatic cells. As necrotic tissue yields to fibrosis, this disease alters liver structure and normal vasculature, impairs blood and lymph flow, and ultimately causes hepatic insufficiency.
Source: Handbook of Medical-Surgical Nursing 3rd Edition by Springhouse, 2006
Liver Cirrhosis Cirrhosis is a consequence of chronic liver disease characterized by replacement of liver tissue by fibrous scar tissue as well as regenerative nodules (lumps that occur as a result of a process in which damaged tissue is regenerated) leading to progressive loss of liver function.
Source: Blackwell’s Dictionary of Nursing 5th Edition, 2004
26
27
PHYSICAL ASSESSMENT
Date and Time Performed: February 11, 2010 at 5:00 pm Personal Data Cutie is a male patient itted to the Med of Davao Medical Center. He is 72 years old and was born on May 23, 1937. He was born in IGACOS, Davao City and is currently living at Buhangin, Davao City. He is Filipino and a Christian (Roman Catholic) in religion. He is married. The reason for his ission is malaise, loss of appetite, nausea, and black stools experienced on the 6th of February, 2010. Health History The patient claimed that he never had any past illnesses that lead him to an ission to a hospital. It was just a number of feverish experiences, cough, colds and flu which he had. It was stated by his wife upon our interview that he was diagnosed with hypertension a year ago and had maintenance medications. And just a month ago, he then had chest pain, dizziness, nausea, and body malaise. General Survey Received lying on bed unconscious as evidenced by the patient not responding to verbal and pain stimuli. Patient had an IVF of D5NaCl at 80cc/hr infusing well at left metacarpal vein; with endotracheal tube with O2 at 5-7 L/min connected to a bag valve; with Foley catheter connected to a Urobag draining 100 cc of dark yellow colored urine. He was untidy as the patient was with dirty feet and untrimmed and dirty nails. 28
Vital Signs: BP- 110/70mmhg
Temperature- 38.3
PR- 96bpm
RR- 24
Skin The patient had jaundice with uniform skin color all throughout the body except under his axillae, which is darker. His skin folds and axillae were moist. Skin temperature was uniform in all extremities when touched. Senile skin was noted. Hair Upon inspection, hair was short and white in color. His hair was thin and evenly distributed as evidenced by the absence of areas of alopecia along the scalp. No infection or infestations were noted upon inspection and palpation of the patient’s hairline and scalp. Dandruff was noted on patient’s scalp however there were no lesions, lumps, or masses upon palpation. Nails Clubbing of nails was noted on patient. Upon palpation, nail base was firm and fingernails had a rough texture. Epidermis surrounding the nails was intact and no lesions were noted. Nails were long, dirty and untrimmed. Toenail surface was slightly curved and rough.
29
Skull and Face Skull was rounded and normocephalic. Symmetry in anatomy of face was noted. Eyes and Vision Hair of eyebrows was evenly distributed and periorbital skin was intact without swelling or inflammation. Eyebrows were symmetrically aligned. Upon inspection, skin of eyelids was intact and no discharges and discolorations were present. Icteric sclera was noted. Iris were black in color, and had a round, smooth border. Pupillary response to illumination was sluggish and equal on both eyes as evidenced by constricting of both illuminated and non-illuminated pupils upon illumination. Patient does not wear glasses: visual acuity when he was still conscious and awake was grossly normal as stated by his wife. Ears and Hearing Upon inspection, auricles were of the same color with facial skin, were symmetrically aligned with each other, and were aligned with the outer canthus of each eye. Cerumen was present but was not impacted or excessive in amount. Upon palpation, auricles were firm, and not tender as evidenced by the auricle being pulled upward, downward, and backward without resistance, and the pinna being folded forward without resistance and recoiling after folding. Patient was unresponsive since he is in comatose.
30
Nose Upon inspection, external nose was symmetrical. No abnormal discharges or flaring were noted. Also, the nose was with uniform color with facial skin. Nasal septum was intact and in midline. Patient was with NGT on his right nares. Mouth Upon inspection, endotracheal tube with O2 at 5-7 L/min connected to bag valve was noted. Outer lips were brownish pink and were dry. Teeth were shiny and yellow in color. Neck Upon inspection, neck veins were not distended or visible. Shoulder muscles were of anatomically symmetrical. Thorax and Lungs The skin over the posterior thorax was intact and uniform in color with the rest of the body. Also, chest expansion was symmetrical when air is istered through the endotracheal tube with O2 at 5-7 L/min connected to a bag valve. Crackles were noted upon auscultation. Cardiovascular and Peripheral Vascular Peripheral pulses were regular and present on all four extremities. Slow capillary refill time of 4-5 seconds gathered upon three checks was noted.
31
Chest No masses, lesions or any unusuality noted on patient’s chest. Abdomen Upon inspection, distended abdomen and ascites was noted. Abdomen was supple when palpated. Size of abdomen was observed to be not appropriate for patient’s body. Abdominal girth of 39 inches was taken. Caput medusae noted on the skin of the abdomen. Genito-urinary Upon inspection, no swelling, lesion or mass noted on the genitals of the patient. Patient is with Foley catheter which is connected to a Urobag draining 100 cc of dark yellow colored urine. Back and Extremities Patient was not able to manifest movements on the upper body and lower body since the patient was not conscious during the assessment. Bones appear to have no deformities. Elbows have no deformities. However a grade 1 pitting edema was noted on all four extremities as skin does not immediately (approximately 4 seconds) go back to its normal state when pressure is applied.
32
ANATOMY AND PHYSIOLOGY
Liver The liver is the largest internal organ in the body, and weighs about 3 pounds in an adult. The liver is located in the right upper quadrant of the abdomen, just below the diaphragm. A thick capsule of connective tissue called Glisson's capsule covers the entire surface of the liver. The liver is divided into a large right lobe and a smaller left lobe. The falciform ligament divides the two lobes of the liver. Each lobe is further divided into lobules that are approximately 2 mm high and 1 mm in circumference. These hepatic lobules are the functioning units of the liver. Each of the approximately 1 million lobules consists of a hexagonal row of hepatic cells called hepatocytes. The hepatocytes secrete bile into the bile channels and also perform a variety of metabolic functions. Between each row of hepatocytes are small cavities called sinusoids. Each sinusoid is lined with Kupffer cells, phagocytic cells that remove amino acids, nutrients, sugar, old red blood cells, bacteria and debris from the blood that flows through the sinusoids. The main functions of the sinusoids are to destroy old or defective red blood cells, to remove bacteria and foreign particles from the blood, and to detoxify toxins and other harmful substances. Approximately 1500 ml of blood enters the liver each minute, making it one of the most vascular organs in the body. Seventy-five percent 33
of the blood flowing to the liver comes through the portal vein; the remaining 25% is oxygenated blood that is carried by the hepatic artery. The hepatic portal system begins in the capillaries of the digestive organs and ends in the portal vein. Consequently, portal blood contains substances absorbed by the stomach and intestines. Portal blood is ed through the hepatic lobules where nutrients and toxins are absorbed, excreted or converted. Restriction of outflow through the hepatic portal system can lead to portal hypertension. Portal hypertension is most often associated with cirrhosis. Patients usually present with splenomegaly, ascites, GI bleeding and/or portal systemic encephalopathy. The consequences of portal hypertension are due to portal systemic anastomosis formed by the body as an attempt to by the obstructed liver circulation. These collateral vessels form along the falciform ligament, diaphragm, spleen, stomach and peritoneum. The collaterals find their way to the renal vein where blood drained from the digestive organs is let into the systemic circulation. The liver is responsible for important functions, including: •
Bile production and excretion
•
Excretion of bilirubin, cholesterol, hormones, and drugs
•
Metabolism of fats, proteins, and carbohydrates
•
Enzyme activation
34
•
Storage of glycogen, vitamins, and minerals
•
Synthesis of plasma proteins, such as albumin and globulin, and clotting factors
•
Blood detoxification and purification
The liver synthesizes and transports bile pigments and bile salts that are needed for fat digestion. Bile is a combination of water, bile acids, bile pigments, cholesterol, bilirubin, phospholipids, potassium, sodium, and chloride. Primary bile acids are produced from cholesterol. When bile acids are converted or "conjugated" in the liver, they become bile salts. Bilirubin is the main bile pigment that is formed from the breakdown of heme in red blood cells. The broken-down heme travels to the liver, where is it secreted into the bile by the liver. Bilirubin production and excretion follow a specific pathway. When the reticuloendothelial system breaks down old red blood cells, bilirubin is one of the waste products. This "free bilirubin" is a lipid soluble form that must be made water-soluble to be excreted. The conjugation process in the liver converts the bilirubin from a fat-soluble to a water-soluble form. The liver also plays a major role in excreting cholesterol, hormones, and drugs from the body. The liver plays an important role in metabolizing nutrients such as carbohydrates, proteins, and fats. The liver helps metabolize carbohydrates in three ways: •
Through the process of glycogenesis, glucose, fructose, and galactose are converted to glycogen and stored in the liver.
35
•
Through the process of glycogenolysis, the liver breaks down stored glycogen to maintain blood glucose levels when there is a decrease in carbohydrate intake.
•
Through the process of gluconeogenesis, the liver synthesizes glucose from proteins or fats to maintain blood glucose levels.
The liver synthesizes about 50 grams of protein each day, primarily in the form of albumin. Liver cells also chemically convert amino acids to produce ketoacids and ammonia, from which urea is formed and excreted in the urine. Digested fat is converted in the intestine to triglycerides, cholesterol, phospholipids, and lipoproteins. These substances are converted in the liver into glycerol and fatty acids, through a process known as ketogenesis. Prothrombin and fibrinogen, substances needed to help blood coagulate, are both produced by the liver. The liver also produces the anticoagulant heparin and releases vasopressor substances after hemorrhage. Liver cells protect the body from toxic injury by detoxifying potentially harmful substances. By making toxic substances more water soluble, they can be excreted from the body in the urine. The liver also has an important role in vitamin storage. High concentrations of riboflavin or Vitamin B1 are found in the liver. 95% of the body's vitamin A stores are concentrated in the liver. The liver also contains small amounts of Vitamin C, most of the body's Vitamin D stores, and Vitamins E and K.
36
Biliary tract The biliary tract (or biliary tree) is the common anatomy term for the path by which bile is secreted by the liver on its way to the duodenum, or small intestine, of most of the mammal family. It is referred to as a tree because it begins with many small branches which end in the common bile duct, sometimes referred to as the trunk of the biliary tree. The duct is present along with the branches of the hepatic artery and the portal vein forming the central axis of the portal triad. Bile flows in opposite direction to that of the blood present in the other two channels. The liver is usually excluded, but sometimes included. Pressure inside in the biliary tree can give rise to gall stone and lead to cirrhosis of the liver. Blockage can cause jaundice. The biliary tract can also serve as a reservoir for intestinal tract infections. Since biliary tract is an internal organ, it has no somatic nerve supply,and,therefore,colicky pain due to infection and inflammation of the biliary tract is not a somatic pain but it may be caused by luminal distension which causes stretching of the wall (the same mechanism of pain in intestinal colic in intestinal obstruction in which intestine also do not have somatic nerve supply)
37
The path is as follows: •
Bile canaliculi >> Canals of Hering >> bile ductules (in portal tracts) >> intrahepatic bile ducts >> left and right hepatic ducts >>
•
merge to form >> common hepatic duct >>
•
exits liver and s >> cystic duct (from gall bladder) >>
•
forming >> common bile duct >> s with >> pancreatic duct >>
•
forming >> ampulla of Vater >> enters duodenum The anatomy of the biliary tree is a little complicated, but it is important to
understand. The liver's cells (hepatocytes) excrete bile into canaliculi, which are intercellular spaces between the liver cells. These drain into the right and left hepatic ducts, after which bile travels via the common hepatic and cystic ducts to the gallbladder. The gallbladder, which has a capacity of 50 milliliters (about 5 tablespoons), concentrates the bile 10 fold by removing water and stores it until a person eats. At this time, bile is discharged from the gallbladder via the cystic duct into the common bile duct and then into the duodenum (the first part of the small intestine), where it begins to dissolve the fat in ingested food. The liver excretes approximately 500 to 1000 milliliters (50 to 100 tablespoons) of bile each day. Most (95%) of the bile that has entered the intestines is resorbed in the last part of the small intestine (known as the terminal ileum), and returned to the liver for reuse.
38
The many functions of bile are best understood by knowing the composition of bile: 1. Bile Salts (cholates, chenodeoxycholate, deoxycholate): these are produced by the liver's breakdown of cholesterol. They function in bile as detergents that dissolve dietary fat and allow it to be absorbed. Hence, disruption of bile excretion disrupts the normal absorption of fat, a process called malabsorption. Patients develop diarrhea because the fat is not absorbed (steatorrhea) , and develop deficiencies of the fat-soluble vitamins (A, D, E, and K). 2. Cholesterol and phospholipids-while only 4% of bile is cholesterol, the secretion of cholesterol and its metabolites (bile salts) into bile is the body's major route of elimination of cholesterol. Phospholipids, which are components of cell membranes, enhance
the
cholesterol
solubilizing
properties of bile salts. Inefficient excretion of cholesterol can cause an increased serum cholesterol. This predisposes to vascular disease (heart attacks, strokes, etc.) 3. Bilirubin-while this comprises only 0.3% of bile, it is responsible for bile's yellow color. Bilirubin is a product of the body's metabolism of hemoglobin, the carrier of oxygen in red blood cells. Disruption of the excretion of this component of bile leads to a yellow discoloration of the eyes and skin (jaundice). 4. Protein and miscellaneous components
39
Bile production and recirculation is the main excretory function of the liver. Tumors that obstruct the flow of bile from the liver can also impair other liver functions. Therefore, it is necessary to understand these other functions to understand the symptoms that these tumors can cause. These include: Metabolic functions, such as the maintenance of glucose (blood sugar) levels Synthetic functions, such as the synthesis of serum proteins such as albumin, blood clotting (coagulation) factors, and complement (a mediator of inflammatory responses) Storage functions, such as the storage of sugar (glycogen), fat (triglycerides), iron, copper, and fat soluble vitamins (A, D, E, and K) Catabolic functions, such as the detoxification of drugs Circulation of the blood in blood vessels There are two circulatory routes of blood as it flows through the blood vessels: the systemic and the pulmonary circulation. In systemic circulation, blood flows from the left ventricle of the heart through blood vessels to all parts of the body (except gas exchange tissues of lungs) and back to the atrium. In pulmonary circulation on the other hand, venous blood moves from the right atrium to right 40
ventricle to pulmonary artery to lung arterioles and capillaries where gases exchanged; oxygenated blood returns to the left atrium via pulmonary veins; from left atrium, blood enters the left ventricle.
Hepatic Portal Circulation The veins of the hepatic portal digestive
circulation organs,
drain
the
spleen,
and
pancreas and deliver this blood to the liver through the hepatic portal vein. When you have just eaten, the hepatic portal blood contains large amounts of nutrients. Since the liver is a key body organ involve in maintaining the proper glucose, fat and protein concentrations in the blood, this system “takes a detour “to ensure that the liver processes these substances before they enter the systemic circulation. As blood flows slowly through the liver, some of the nutrients are removed to be stored or processed in various ways for later release to the blood. The liver is drained by the hepatic veins that enter the inferior vena cava. Like the portal circulation that links the hypothalamus of the brain and the anterior pituitary gland, the hepatic portal circulation is
41
a unique and unusual circulation. Normally, arteries feed capillary beds, which in turn drain into veins. Here we see veins feeding the liver circulation. The inferior mesenteric vein, draining the terminal part of the large intestine, drains into the splenic vein, which itself drains the spleen, pancreas and the left side of the stomach. The splenic vein and superior mesenteric vein (which drains the small intestine and the first part of the colon) to form the hepatic portal vein. The L. Gastric vein, which drains the right side of the stomach, drains directly into the hepatic portal vein.
42
ETIOLOGY
43
Basic Etiology Predisposing
Present/
Rationale
Actual
Absent
Factors Male
Liver Cirrhosis occurs
The patient is male.
mostly in men. http://www.cancer.org/docr oot/cri/content/cri_2_2_2x_ what_causes_liver_cancer_ 25.asp Ages 45-75
Liver Cirrhosis is most
The patient is 72 years old.
common among people ages Race: Asian
45-75 years old. In Asia and Africa, cirrhosis
The patient is an Asian since
is also common but more
he was born from Filipino
likely to be associated with
parents, and he was born in
hepatitis.
IGACOS, Davao City, and currently resides here in
http://esynopsis.uchc.edu/e
Buhangin, Davao City.
Atlas/GI/1210.htm
Biliary atresia
X
Infants can be born without
The patient has no record or
bile ducts (biliary atresia)
history of Biliary atresia.
and ultimately develop cirrhosis. The bile ducts carry bile formed in the liver to the intestines, where the bile helps in the digestion of fat. So, when the bile ducts are blocked, bile is trapped in the liver, http://www.medicinenet.co m/cirrhosis/page3.htm
44
Basic Etiology Precipitating
Present/
Rationale
Actual
Absent
Factors Chronic
alcoholism
Chronic high levels of alcohol
As stated by the
consumption injure liver cells.
patient’s wife, the
Alcohol seems to injure the liver
patient at his young age
by blocking the normal
was able to drink 1 long
metabolism of protein, fats, and
neck (750 ml) of
carbohydrates. Alcohol can
Tanduay on his own. At
poison all living cells, causing
times, he goes beyond 1
liver cells to become inflamed
long neck and even
and die. Thirty percent of
drinks half a gallon of
individuals who drink daily at
“Tuba” when he is not
least eight to sixteen ounces of
yet drunk. As stated by
hard liquor or the equivalent for
his wife, his husband
fifteen or more years will develop
does not stop drinking
cirrhosis.
unless he becomes drunk. When he reached
http://www.emedicinehealth.com/ cirrhosis/page2_em.htm#Cirrhosi s%20Causes
his adulthood, he continues to drink and smoke when he finds time to do them.
Chronic viral
X
Condition where hepatitis B or
The patient had no
hepatitis
hepatitis C virus infects the liver
medical record of
(types B, C,
for years. some patients infected
acquiring hepatitis B, C,
and D).
with hepatitis B virus and most
or D.
patients infected with hepatitis C virus develop chronic hepatitis, which, in turn, causes progressive
45
liver damage and leads to cirrhosis, and, sometimes, liver cancers. Hepatitis B causes liver inflammation and injury that over several decades can lead to cirrhosis. Hepatitis D is dependant on the presence of hepatitis B, but accelerates cirrhosis in co-infection The hepatitis C virus ranks with alcohol as a major cause of chronic liver disease and cirrhosis. Infection with this virus causes inflammation of and low grade damage to the liver that over several decades can lead to cirrhosis. http://www.spiritustemporis.com/cirrhosis/causes.ht ml
46
Smoking
Research reveals that smoking
The patient smokes 1-2
damages the liver. Smoking
packs of cigarette a day,
activates chemical materials
and he started smoking
within the body. These chemicals
when he was a teenager.
that are manufactured by smoking At the same time, he also provoke oxidative stress
also drinks Tanduay
which is linked with lipid
(750mL) 2-3 times a
peroxidation. When this occurs,
week since he was a
the condition fibrosis is
teenager. He only
developed.
stopped smoking when
Smoking increases the manufacturing of pro-
he was diagnosed with hypertension last 2009.
inflammatory cytokines which is related to liver cell damage. Smoking also contributes the continued succession of chronic alcoholic-hepatitis as well as to the progression of cirrhosis.
Http://www.ehow.com/howdoes_4577854_effects-smokingdrinking-liver.html
47
Malnutrition, especially
X
Fat builds up in the liver and
There is no scientific
eventually causes cirrhosis.
basis that the patient has
high fat intake
an increase fat in the Fat (triglycerides) accumulates throughout the hepatocytes for the following reasons: •
Export of fat from the
blood or increased level of cholesterol in the blood (LDL-bad cholesterol)
liver is decreased because hepatic fatty acid oxidation and lipoprotein production decrease. •
Input of fat is increased because the decrease in hepatic fat export increases peripheral lipolysis and triglyceride synthesis, resulting in hyperlipidemia.
http://digestive.niddk.nih.gov/ddi seases/pubs/cirrhosis/
48
SYMPTOMATOLOGY
SYMPTOMS
Present/
Rationale
Actual
absent Anorexia
Increased brain tryptophan (TRP)
This is present
availability for serotonin synthesis
with the patient,
play a role in the pathogenesis of
since this is one
anorexia. Since in chronic liver
of the reasons he
failure, increased plasma and
consulted the
cerebrospinal fluid TRP
emergency room.
concentrations are characteristically
The wife stated
reported, that also in liver cirrhosis,
that the patient
increased brain TRP availability
had no appetite to
constitute the pathogenic mechanism
eat
of anorexia.
http://www3.interscience.wiley.com/j ournal/49716/abstract? CRETRV=1&SRETRY=0 Nausea and vomiting
The malabsorption of fats may lead
Two weeks prior
to deficit of fatsoluble vitamins,
to ission, the
hemorrhoids, intolerance to fatty
patient started
foods, nausea and vomiting attacks,
feeling nauseous,
and abdominal bloating. Since the
and four days
liver has already decreased in
prior to
function, its function to produce bile
ission, he had
which emulsifies fats is also
prandial vomiting
decreased, thus these symptoms
which is one of
persists.
the reasons he
49
www.enwikipedia.org/wiki/Liver_dis
sought
ease#Symptoms_of_a_diseased_liver
consultation at the emergency room.
Body malaise
This is due to the decreased in liver
The patient
function of the liver because of the
experienced body
hepatic fibrosis. Therefore, the
malaise, and was
patient has also decreased
one of his chief
erythropoietin which then results to
complaint that
the decrease of red blood cells
resulted to his
circulating in the blood, and there
ission at
will be decreased hemoglobin. All of
DMC.
this in return will cause the patient to have body malaise. Bleeding
tendencies
Bleeding tendencies such as
The patient had
nosebleeds, easy bruising, and
bleeding as
bleeding gums may result from
evidenced by him
thrombocytopenia secondary to
having black
splenomegaly, decreased vitamin K
stools, which is
absorption and decreased production
also known as
of coagulation factors and
melena, indicative
regurgitation of blood to the spleen
of bleeding in the
and gastrointestinal tract.
upper gastrointestinal tract.
Suddarth, Doris Smith. The Lippincott Manual of Nursing Practice. 5th edition. 1991. Pages 514515.
Portal
Portal hypertension occurs because of The patient has
50
hypertension
the obstruction of portal circulation
ascites which is a
brought about by the portal
complication of
obstruction caused by the hepatic
portal
scarring.
hypertension.
http://www.emedicinehealth.com/cirr hosis/page2_em.htm#Cirrhosis %20Causes
This is an evidence that he indeed has portal hypertension. In addition, the patient was diagnosed to have hypertension on the year 2009.
Ascites
This
happened
because
of
the The patient has
decrease of albumin in the blood ascites as plasma. Albumin is responsible for evidenced by his maintaining the oncotic pressure in distended the blood volume. A decrease in abdominal cavity. albumin will mean a decrease in oncotic pressure, which will result to a more permeable membrane which results to fluid leaking through the vasculature
into
the
abdominal
cavity. Suddarth, Doris Smith. The Lippincott Manual of Nursing Practice. 5th edition. 1991. Pages 514515. Jaundice
Jaundice is the buildup of bile
The patient was
pigment that is ed by the liver
noted to have 51
into the intestine. Due to the portal
yellowish skin
obstruction, the bile going to the GI
color on all four
tract will have a backflow to the
extremities
liver. The bile then goes to the blood
including the
stream, and this causes the yellowing
palms. The
of the skin, due to the presence of bi
patient also had icteric sclera
(http://www.healthscout.com/ency/68
when inspected.
/292/main.html)
edema on the
extremities
Plasma albumin is reduced, leading One week prior to to edema.
ission, the wife of the patient
Suddarth, Doris Smith. The
noticed the
Lippincott Manual of Nursing
obvious
Practice. 5th edition. 1991. Pages 514- abdominal 515.
distention of the patient’s abdomen. Upon physical assessment, the patient was noted to have ascites and edema on all four extremities.
Caput medusae
Portal hypertension results from the
The patient was
abnormal blood flow pattern in liver
noted to have
created by cirrhosis. The increased
large, dilated, and
pressure is transmitted to collateral
distended veins
venous channels. Sometimes these
on the abdomen
venous collaterals are dilated. Caput
area when
52
medusa consists of dilated veins seen
inspected
on the abdomen of a patient with cirrhosis of the liver.
Coma
This is a progressive symptom, The patient is on a secondary to the loss of ammonia to comatose state. urea
conversion
and
consequent
delivery of toxic ammonia to the brain. Deterioration of mental function from lethargy to coma and eventual death
PATHOPHYSIOLOGY
53
PATHOPHYSIOLOGY
54
DOCTOR’S ORDERS DATE
DOCTOR'S
RATIONALE
REMARKS
ORDER Feb. 6,
Please it patient ission in the hospital is required
2010
under blue service – for optimum medical and nursing care;
ITTED
55
Level II Pavillion and to receive medications, undergo tests, and perform procedures which can only be done in the hospital setting. The blue service accommodates patients with gastro, endo and immunologic problems. VSq4 and record
Vital signs are taken to provide
TAKEN
please
baseline data and to watch-out for any
AND
unusualities.
RECORDED
Start venoclysis with Helps expand intravascular volume, PNSS 1L @
corrects an underlying imbalance in
120cc/hr
fluids and electrolytes and compensates
STARTED
the loss in the body. Moreover, it serves as a route for medication. Labs:
CBC (complete blood count and
CBC PC
platelet count) is a basic screening test WITH and is one of the most frequently
DONE
RESULTS
ordered laboratory procedures. The findings in the CBC PC give valuable diagnostic information about the hematologic and other body systems, prognosis, response to treatment and recovery. CXR-PA
A chest radiograph is used to diagnose DONE BUT
56
conditions affecting the chest, its
NO
contents, and nearby structures. Chest
IMPRESSIO
radiographs are among the most
N MADE
common films taken, being diagnostic of many conditions. A chest x-ray may be ordered when a person's symptoms include a persistent cough, coughing up blood, chest pain, a chest injury, or difficulty in breathing. ECG
ECG is a non-invasive test used to
NOT DONE
assess the heart function. It is a graphic produced by an electrocardiograph, which records the electrical activity of the heart over time. B1 B2
Elevation of serum bilirubin levels is
DONE
related to hemolysis of RBCs and
WITH
subsequent re-absorption of
RESULTS
unconjugated bilirubin from the small intestines. The condition may be benign or may place the patient at risk for multiple complications/untoward effects.
57
BUN
The BUN test is primarily used, along DONE with the creatinine test, to evaluate
WITH
kidney function in a wide range of
RESULTS
circumstances, to help diagnose kidney disease, and to monitor patients with acute or chronic kidney dysfunction or failure. Increased BUN levels suggest impaired kidney function. This may be due to acute or chronic kidney, damage, or failure. S. Na, S. K
Serum sodium and serum potassium
NOT DONE
levels are checked to determine fluid and electrolyte balance. Crea
A disorder in the kidney function
NOT DONE
reduces excretion of creatinine, resulting in increased blood creatinine levels. This test diagnoses impaired renal functions. SGPT and SGOT
Elevations of SGPT, an enzyme found DONE within the liver cells, indicate that the WITH liver cells are either leaky (internal
RESULTS
contents are entering the blood) or damaged.
58
Meds:
Inhibits reabsorption of sodium and
Furosemide 40 mg
chloride at proximal and distal tubule
tab OD
and in the loop of Henle
Spironolactone
Spironolactone inhibits the action of
25mg tab OD
aldosterone thereby causing the kidneys
GIVEN
GIVEN
to excrete salt and fluid in the urine while retaining potassium. Essentiale Forte
Increase functional status of the liver,
CAP BID
improvement in the lipids metabolism
GIVEN
caused by accelerated synthesis of lipoproteins in the liver, activation of the phospholipid-depending ferments, increased synthesis of glycogen in the liver, decreased the fatty infiltration of the hepatocytes I&O q shift
Intake & output monitoring is done to
RECORDED
assess the fluid retention status of the patient and to prevent cardiac overload. Watch out for any
To ensure that immediate nursing
WATCHED
unsualities
interventions can be rendered in cases
OUT
of deviances from the normal health status so complications can be prevented Refer accordingly
Referral is done to correct unusualities
REFERRED
as soon as possible and to inform the
59
attending physician of the patient's condition. February Labs: CBC PC,
These tests were not yet done and so
7, 2010
ECG, B1 B2, S. Na, the doctor ordered again and made
@ 4:00
K, Crea, SGPT,
AM
SGOT
NOT DONE
requests for these tests for analysis.
Follow up chest X-
This is to inform the patient or
FOLLOWED
ray reading
significant other to have the copy of the UP result from the laboratory.
Additional labs: 1.
Transabdominal USD is ordered to for NOT DONE
Transabdominal
visualization of the abdomen which
USD
helps in diagnosing the patient’s condition.
2. Serum albumin
A serum albumin test measures the
DONE
amount of this protein in the clear
WITH
liquid portion of the blood. This test
RESULTS
can help determine if a patient has liver disease or kidney disease, or if the body is not absorbing enough protein. 3. HBS-Ag
The hepatitis B surface antibody (anti- NOT DONE HBs) is the most common test. Its presence indicates previous exposure to HBV, but the virus is no longer present and the person cannot on
60
the virus to others. 4. Anti-HAV IgM
This test is used to help diagnose a
NOT DONE
liver infection due to the hepatitis A virus (HAV). This test may also be used to determine if you have produced antibodies and developed immunity in response to a hepatitis A vaccine or a previous hepatitis A infection. 6. Anti-HCV
To determine if you have contracted
NOT DONE
the hepatitis C virus (HCV) and to monitor treatment of the infection 7. PT/PTT
Since the Prothrombin time (PT)
NOT DONE
evaluates the ability of blood to clot properly, it can be used to help diagnose bleeding. When used in this instance, it is often used in conjunction with the PTT to evaluate the function of all coagulation factors. Occasionally, the test may be used to screen patients for any previously undetected bleeding problems prior to surgical procedures.
61
Furosemide 40mg
Inhibits reabsorption of sodium and
IVTT now, then
chloride at proximal and distal tubule
GIVEN
Furosemide 40mg 1 and in the loop of Henle tab BID Spironolactone
Spironolactone inhibits the action of
100mg BID
aldosterone thereby causing the kidneys
GIVEN
to excrete salt and fluid in the urine while retaining potassium. Essentiale Forte 1
Increase functional status of the liver,
cap TID
improvement in the lipids metabolism
GIVEN
caused by accelerated synthesis of lipoproteins in the liver, activation of the phospholipid-depending ferments, increased synthesis of glycogen in the liver, decreased the fatty infiltration of the hepatocyte Lactulose 30cc @
Produces osmotic effect in colon.
bedtime
Resulting distention promotes
GIVEN
peristalsis. Decrease blood ammonia build- up causes hepatic encephalopathy, probably ass result of bacterial degradation which lowers pH of colon contents. Ceftriaxone 1gm
This antimicrobial agent inhibits
GIVEN
62
IVTTq12, ANST
bacterial cell wall synthesis by binding to one or more of the penicillinbinding proteins (PBPs) which in turn inhibits the final transpeptidation step of peptidoglycan synthesis in bacterial cell walls, thus inhibiting cell wall biosynthesis. Bacteria eventually lyse due to ongoing activity of cell wall autolytic enzymes (autolysins and murein hydrolases) while cell wall assembly is arrested.
Please monitor I&0
Intake & output monitoring is done to
MONITORE
q shift and record
assess the fluid retention status of the
D
patient and to prevent cardiac overload. Refer if UO < 30
A decrease in urine output may indicate REFERRED
cc/hr
a serious, even life-threatening condition. It may be caused by dehydration du, diarrhea, lack of adequate fluid intake or total urinary tract obstruction.
CBG q6 (6AM-
The capillary blood glucose test is
11AM- 6PM –
ordered to measure the amount of
11PM)
glucose in the blood right at the time
NOT DONE
of sample collection. It is used to
63
detect both hyperglycemia and hypoglycemia , to help diagnose diabetes, and to monitor glucose levels. Refer if CBG ≥
High levels of glucose most frequently REFERRED
180mg/dL, <
indicate diabetes, but many other
80mg/dL
diseases and conditions can also cause elevated glucose such as chronic renal failure and hyperthyroidism. Low blood glucose levels are seen in patients with drinking alcohol and extensive liver disease.
Refer
Referral is done to correct unusualities
REFERRED
as soon as possible and to inform the attending physician of the patient's condition. February Please do gastric
Gastric lavage is done to address
7, 2010
lavage now until
gastrointestinal bleeding.
@ 8:10
water is clear
AM
DONE
Please insert FBC
To monitor the intake and output of the INSERTED
F16 and attach to
patient. This may also avoid bladder
urobag
distention.
64
Strict I&O
Intake & output monitoring is done to
MONITORE
monitoring and
assess the fluid retention status of the
D AND
record please
patient and to prevent cardiac overload. RECORDED
NPO Temporarily
For better visualization of the abdomen DONE during the ultrasound
Shift IVF to D5NSS D5NSS restores sodium chloride deficit SHIFTED 1L @ 80cc/hr
and extra cellular fluid volume.
For USD of the
Abdominal ultrasound is an imaging
whole abdomen,
procedure used to examine the
KUB, Pancreas
presence of abnormalities in the
NOT DONE
structure of the organs intraabdominally. Continue other meds All medications previously ordered by attending physician should be
CONTINUE D
continued to hasten patient's recovery. Please attach all labs For monitoring and analysis of the requested
ATTACHED
patient’s condition through the results of the tests done
Feb. 8,
Start omeprazole
Suppress gastric acid secretion by
2010 @
40mg IVTTq12, 1st
inhibiting the partial cell H+/K+ ATP
6:20 AM done once available
STARTED
pump
*coffeeground output / NGT 65
Feb. 9,
Repeat CBC,
These tests were not yet done and so
2010 @
protime, USD of the the doctor ordered again and made
11:00
liver, Pancreas,
AM
serum albumin,
NOT DONE
requests for these tests for analysis.
BUN Lactulose 30cc TID, Produces osmotic effect in colon. to make 4-5 bowl
Resulting distention promotes
mvt/day
peristalsis. Decrease blood ammonia
GIVEN
build- up the causes hepatic encephalopathy, probably ass result of bacterial degradation which lowers pH of colon contents. Furosemide 40 mg
Inhibits reabsorption of sodium and
IVTT, OD
chloride at proximal and distal tubule
GIVEN
and in the loop of Henle Omeprazole 40mg
Suppress gastric acid secretion by
IVTT q12
inhibiting the partial cell H+/K+ ATP
GIVEN
pump Vit. K 1 amp IVTT
It is given to prevent bleeding.
GIVEN
OD Essential Forte 1 cap Increase functional status of the liver, TID
GIVEN
improvement in the lipids metabolism caused by accelerated synthesis of lipoproteins in the liver, activation of the phospholipid-depending ferments,
66
increased synthesis of glycogen in the liver, decreased the fatty infiltration of the hepatocytes Metronidazole
Disrupts DNA and protein synthesis
500mg 1 TAB q6
susceptible organisms. Therapeutic
GIVEN
effects: Bactericidal, trichomonacidal or amebicidal action. Spectrum: Most notable for avtivity against anaerobic bacteria including: Bacteroides, clostridium. In addition is active against: Trichomonas vaginalis, entamoeba histolytica, giardia lamdia, H. pylori and clostridium difficile. Hold all PO Meds
Holding all PO meds is done as
DONE
preparation for the gastric lavage. Giving medications would just be drawn out of the patient’s stomach during the procedure. Pls. do gastric lavage Gastric lavage is done to address
DONE
until gastric aspirate gastrointestinal bleeding. goes out clear NPO temporarily
For better visualization of the abdomen DONE during the ultrasound
CBG Monitoring q6 The capillary blood glucose test is ordered to measure the amount of
NOT MONITORE
67
glucose in the blood right at the time
D
of sample collection. It is used to detect both hyperglycemia and hypoglycemia , to help diagnose diabetes, and to monitor glucose levels. Refer for persistent ↓ To notify the physician regarding the in sensorium
REFERRED
changes of the patient’s health status and to prevent further complications
Feb. 9,
Restrain if necessary Patient may be restless or
2010 @ (per watcher’s
uncomfortable with the equipment
12:05
attached to him needing a restraint to
request)
PM
RESTRAINE D
keep them in place and prevent dislodging causing harm.
Feb. 10, Repeat CBC Plt Ct,
These tests were not yet done and so
2010 @
Protime with INR,
the doctor ordered again and made
1PM
Serum Na, K, Crea,
requests for these tests for analysis.
ABG
Blood gases are a measurement of
NOT DONE
DONE
how much oxygen and carbon dioxide is in your blood. It also determines the acidity (pH) of your blood. The test is used to evaluate respiratory diseases and conditions that affect the lungs. It helps determine the effectiveness of
68
oxygen therapy. The test also provides information about the body's acid/base balance, which can reveal important clues about lung and kidney function and the body's general metabolic state. Please facilitate
To conduct ultrasound testing to the
FACILITAT
transport on USD
patient which may be helpful in
ED
test today
determining other problems in the patient’s health status
NPO temporarily
For better visualization of the abdomen DONE during the ultrasound
Give tranexamic
Inhibits activation of plasminogen,
GIVEN
acid 100mg IVTT q8 thereby preventing the conversion of plasminogen to plasmin Give Vit. K 1 amp
It is given to prevent bleeding.
GIVEN
now, OD For gastric lavage
This is to ensure that the patient would DONE
today without fail
undergo the gastric lavage as it is needed by the patient immediately on the same day as per doctor’s request
NPO except meds
Restrictions for any intake per orem
DONE
except the medications is given for better visualization of the abdomen during the ultrasound and for patient’s
69
recovery through the therapeutic effects of medicine. Start albumin 25%
To compensate for the decreased
50 cc q12
albumin levels which is responsible for
STARTED
maintaining osmotic pressure inside the blood vessels BP monitoring qh
To monitor changes in the blood
MONITORE
until stable
pressure which is significant in
D
determining the patient’s status Continue meds
All medications previously ordered by
CONTINUE
attending physician should be
D
continued to hasten patient's recovery. Refer
Referral is done to correct unusualities
REFERRED
as soon as possible and to inform the attending physician of the patient's condition. Feb, 10, Referred for ↓
Glasgow Coma Scale or GCS, is
2010
sensorium, (E1 V3
neurological scale which aims to give
M5) GCS 9
a reliable, objective way of recording
CR – 90
the conscious state of a person, for
RR – 22
initial as well as subsequent
T- 39
assessment. (E1 – does not open eyes,
REFERRED
V3- Utters inappropriate words, M5 Localizes painful stimuli) Moderate Brain Injury, GCS 9 – 12
70
Do ABG now
Blood gases are a measurement of
DONE
how much oxygen and carbon dioxide is in your blood. It also determines the acidity (pH) of your blood. The test is used to evaluate respiratory diseases and conditions that affect the lungs. It helps determine the effectiveness of oxygen therapy. The test also provides information about the body's acid/base balance, which can reveal important clues about lung and kidney function and the body's general metabolic state. Do CBG now
The capillary blood glucose test is
NOT DONE
ordered to measure the amount of glucose in the blood right at the time of sample collection. It is used to detect both hyperglycemia and hypoglycemia , to help diagnose diabetes, and to monitor glucose levels. O2 inhalation @ 5-7 O2 inhalation is indicated for patients
DONE
L/min via face mask that lack oxygen supply and need assistance in maintain the desired
71
oxygen supply Monitor VS qh and
The patient is for close monitoring and MONITORE
record
needs further assessment to monitor to D address if there’s any unusualities
Refer
Referral is done to correct unusualities
REFERRED
as soon as possible and to inform the attending physician of the patient's condition. Feb. 11, Follow-up requested For monitoring and analysis of the
FOLLOWED
2010
-UP
labs
patient’s condition through the results of the tests done
For gastric lavage
Gastric lavage is done to address
DONE
gastrointestinal bleeding. Cold water is used to prevent any bleeding in the gastrointestinal tract. IVF of PNSS 1L @
Helps expand intravascular volume,
80cc/hr
corrects an underlying imbalance in
DONE
fluids and electrolytes and compensates the loss in the body. Moreover, it serves as a route for medication
PNSS is isotonic with the blood and tissue fluid, used as a solvent for drugs that are to be istered parenterally
72
like blood to replace body fluids. It is used as a prime once on blood transfusion. Refer
Referral is done to correct unusualities
REFERRED
as soon as possible and to inform the attending physician of the patient's condition. Feb. 11, Referred due to dec. Glasgow Coma Scale or GCS, is 2010
sensorium GCS5 (E1 neurological scale which aims to give
(+)
V1 M3) & dyspnea
REFERRED
a reliable, objective way of recording
active
the conscious state of a person, for
bleeding
initial as well as subsequent
per orem
assessment. E1- Does not open eyes, V1 - Makes no sounds, M3 -
(+) gross
Abnormal flexion to painful stimuli
hematuri
(decorticate response), GCS of 5 –
a on FC
Severe Brain Injury Intubate pt. now
The ET tube is inserted into a
with ET size 75 level patient's trachea in order to ensure that 21
INTUBATE D
the airway is not closed off and that air is able to reach the lungs. The endotracheal tube is regarded as the most reliable available method for protecting a patient's airway.It is
73
indicated when the oxygenation with noninvasive methods is inadequate CAB while awaiting This is to provide the patient with
DONE
mech. vent. adequate oxygen supply through continues bag valving until the mechanical ventilation is available. MV Set-up
To assist the patient in his breathing
PO2 = 100%
pattern since he is not able to
RR 16
his own required oxygen levels.
DONE
TV 500cc Insert NGT French
Nasogastric intubation is a medical
INSERTED
16 and open to drain process involving the insertion of a plastic tube (nasogastric tube, NG tube) through the nose, past the throat, and down into the stomach. The main use of a nasogastric tube is for feeding and for istering drugs and other oral agents. NPO Temp
For better visualization of the abdomen DONE during the ultrasound
Give tranexamic
Inhibits activation of plasminogen,
acid 500mg IVTT
thereby preventing the conversion of
GIVEN
plasminogen to plasmin
74
Vit. K 1amp IVTT
It is given to prevent bleeding.
GIVEN
Suction catheter –
To remove retained secretion in the
SUCTIONE
PRN
catheter to clear obstructed airway
D
Turn to sides q2
Turning the patient to sides prevents
DONE
now – hold
the patient from developing decubitus ulcer. Continue meds
All medications previously ordered by
CONTINUE
attending physician should be
D
continued to hasten patient's recovery. Refer
Referral is done to correct unusualities
REFERRED
as soon as possible and to inform the attending physician of the patient's condition. Feb. 11, Transfer to 6 or 9 To provide better care and monitoring
TRANSFER
2010 @
awaiting for ICU
to the patient while awaiting for room
RED
12NN
vacancy
vacancy in the ICU
For referral to
For co-management and thorough
consultant c/o Dr.
analysis of the patient’s condition.
INFORMED
Honcoda today To receive 2U PRBC In order to increase the number of red
TRANSFUS
and transfuse once
blood cells in the blood
ED
To secure 6U FFP
For the treatment of deficiencies of
SECURED
and transfuse once
coagulation proteins for which specific
available
factor concentrates are unavailable or
available
75
undesirable. Give tranexamic
Inhibits activation of plasminogen,
acid 500mg IVTT
thereby preventing the conversion of
q8, 1 dose now
plasminogen to plasmin
For gastric lavage
Gastric lavage is done to address
with cold water
gastrointestinal bleeding. Cold water
GIVEN
DONE
is used to prevent any bleeding in the gastrointestinal tract. Referral to Dr.
For co-management and thorough
Pilapil
analysis of the patient’s condition.
For HBS-AG, Anti-
These tests were not yet done and so
HBC IgM, Anti-
the doctor ordered again and made
HCV
requests for these tests for analysis.
For USD of the
Abdominal ultrasound is an imaging
whole ABD
procedure used to examine the
REFERRED
NOT DONE
NOT DONE
presence of abnormalities in the structure of the organs intraabdominally. Pls. facilitate transfer To provide better care to the patient in
FACILITAT
to IMCU/ICU
ED
a setting where he will monitored thoroughly.
Feb. 11, Paracetamol 300mg
Inhibits the synthesis of prostaglandins GIVEN
2010 @
that may serve as mediators of pain and
12:45P
IVTT now
fever, primarily in the CNS.
76
M
Refer
Referral is done to correct unusualities
REFFERED
as soon as possible and to inform the T – 38.2
attending physician of the patient's condition.
Feb. 12, Dx: HBS-Ag, Anti-
These tests were not yet done and so
2010 @
the doctor ordered again and made
HBC, Anti-HCV
11:45 AM
DONE
requests for these tests for analysis. Still for mech. vent.
To provide the patient with adequate
amount of oxygen
Follow up
For compatibility testing.
FOLLOWED
crossmatching of
Crossmatching is important to detect
-UP
blood and transfuse
agglutination of donor RBC’s caused
once available
by antibodies in patient's serum.
For compliance to
Continuation of medication ensure INFORMED
medication
spontaneous condition
treatment
and
of
compliance
DONE
patients to
the
medical regimen, revealing the desired outcomes Refer
Referral is done to correct unusualities
REFERRED
as soon as possible and to inform the attending physician of the patient's condition.
77
DIAGNOSTIC EXAMS Arterial Blood Gas Arterial Blood Gas Test is done to determine an imbalance in the amount of oxygen gas (O2) or carbon dioxide gas (CO2) in your blood or an acid-base imbalance, which may indicate a respiratory (lung/breathing), metabolic, or kidney disorder. Blood gas tests are ordered when there are symptoms of an O2/CO2 or pH imbalance, such as difficulty breathing or shortness of breath. Date ordered: February10, 2010
pH
Value
Normal Range
Unit
7.510
7.35-7.45
mmHg
Clinical Significance
Increase in pH is brought about by the increase in bilirubin in the blood which is alkalinic.
pC02
21.3
35-45
mmHg
Decreased pC02 is caused by hypoxia due to the accumulated fluid in the abdominal cavity creating pressure in the diaphragm. Thus, affecting the respiratory status of the patient.
PO2
82.0
80-100
mmHg
PO2 level is at normal range.
78
HC03
16.6
22.0-27.0
mmol/L
When bicarbonate levels are lower than normal, it suggests that the body is having trouble maintaining its acid-base balance. Bicarbonate concentrations in the serum may fall due to consumption by combining with protons (H+) from acids such as lactic acid, keto-acids etc; or by loss from the body from gastro-intestinal or renal sources. Renal loss of bicarbonate may be due to compensatory mechanisms for a respiratory alkalosis.
02Sat
97.2%
80-100
%
02 Saturation is at normal range.
Partially Compensated Respiratory alkalosis Respiratory alkalosis is a medical condition in which increased respiration (hyperventilation) elevates the blood pH (a condition generally called alkalosis). Respiratory alkalosis is due to the dyspnea caused by the pressure exerted by the ascites to the diaphragm, leading to respiratory rate which is lower than normal. Moreover, respiratory alkalosis could result from a ventilatory rate or tidal volume that is too high or from the patient triggering excessive additional breaths.
79
Nursing Responsibilities when withdrawing blood o
order and patient identity
o Explain to the patient the purpose of the hematology or blood test. o
Gather equipment and wear clean gloves
o Inform the patient that the blood sample will be drawn from his antecubital vein in either of the arms. o Apply hot or cold compress to injection site if swelling occurs. o Inform the patient that a total of 5cc of blood will be extracted from him. o Label the sample and maintain chain of custody and deliver or send sample to the lab o Properly dispose of used equipment
80
Hematology
Hematology is the study of blood and its disorders. Hematologists, board-certified internists, look specifically at blood components such as blood count, and blood and bone marrow cells. Hematology tests can help diagnose anemia, hemophilia, blood-clotting disorders, and leukemia. Date ordered: February 6, 2010
81
TEST
RATIONALE
REFERENCE RESULT
N/H/L CLINICAL SIGNIFICANCE
RANGE CBC+PLT Hgb
Hemoglobin is the protein molecule
115-175 g/L
104
L
Low hemoglobin is referred to
in red blood cells that carries oxygen
as anemia which may by the
from the lungs to the body's tissues
decreased erythropoietin caused by
and returns carbon dioxide from the
cirrhosis of the liver.
tissues to the lungs. Hemoglobin also plays an important role in maintaining Hct
RBC count
the shape of the red blood cells. Hematocrit is a measure of how much
0.36-0.52
0.29
L
Because of the decrease in the RBC
space red blood cells take up in the
in the blood, hematocrit as well
blood.
would decrease.
RBC count is the number of red blood 4.20-6.10 cells per volume of blood, and is
2.94
L
x106 /uL
A decreased number of RBCs results from the decrease erythropoietin
reported in either millions in a
production of the liver.
microliter or millions in a liter of blood. WBC count
Measures the amount of white blood
5.0-10.0 x103
cells. These immune cells form in
/uL
9.65
N
WBC is in normal range.
the bone marrow to help fight infection DIFFERENTIAL COUNT
82
83
TEST
RATIONALE
REFERENCE RESULT
N/H/L CLINICAL SIGNIFICANCE
RANGE CBC+PLT Hgb
Hemoglobin is the protein molecule
115-175 g/L
107.0
L
Low hemoglobin is referred to
in red blood cells that carries oxygen
as anemia which may by the
from the lungs to the body's tissues
decreased erythropoietin caused by
and returns carbon dioxide from the
cirrhosis of the liver.
tissues to the lungs. Hemoglobin also plays an important role in maintaining Hct
RBC count
the shape of the red blood cells. Hematocrit is a measure of how much
0.36-0.52
0.31
L
Because of the decrease in the RBC
space red blood cells take up in the
in the blood, hematocrit as well
blood.
would decrease.
RBC count is the number of red blood 4.20-6.10 cells per volume of blood, and is
3.08
L
x106 /uL
A decreased number of RBCs results from the decrease erythropoietin
reported in either millions in a
production of the liver.
microliter or millions in a liter of blood. WBC count
Measures the amount of white blood
5.0-10.0 x103
cells. These immune cells form in
/uL
12.78
H
High levels indicate presence of bacterial infection.
the bone marrow to help fight infection DIFFERENTIAL COUNT
84
Date ordered: February 9, 2010
85
Blood Chemistry Blood chemistry is the chemical composition of the blood. The levels of various substances in the blood can provide clues to a patient's condition, ranging from the presence of a liver disorder to a pregnancy. Routine bloodwork to check blood chemistry is often a part of a diagnostic workup, with the blood being analyzed to check for specific elements which could contribute clues to the diagnosis. Doctors rely on information about normal ranges of things like proteins and lipids to read the blood analysis. Date ordered: February 9, 2010 TEST
RESULT
UNIT
NORMAL
L/N/H
CLINICAL SIGNIFICANCE
L
Low total protein levels can
RANGE TOTAL PROTEIN
59.40
g/L
63 - 82
suggest a liver disorder. In Total protein measurements can reflect
patients with liver problems,
nutritional status and may be used to
there is a decrease in total
screen for and help diagnose kidney
protein levels because of the
disease, liver disease, and many other
decrease in production of
conditions
albumin, a protein which is
86
exclusively produced in the liver. GLOBULIN
40.70
g/L
23 - 35
H
An elevation in the level of serum globulin can indicate the
Globulins are proteins that include
presence of cirrhosis of the liver
gamma globulins (antibodies) and a
and bacterial infection.
variety of enzymes and carrier/transport proteins. They are a diverse group of proteins in the blood, and together represent the second most common proteins in the bloodstream. ALBUMIN
18.70
g/L
35 - 50
L
There is a decrease of albumin in the blood plasma because of
Albumin is the most abundant protein
the decrease in its production
found in blood plasma, representing 40
due to problems in the liver.
to 60% of the total protein. A/G RATIO
0.5
-
1.5 – 2.5
L
A decrease in Albumin
87
Globulin Ratio is an indicative The ratio of the concentrations of
of a problem in liver functions.
albumin to globulin in blood serum.
88
Blood Chemistry Date ordered: February 6, 2010
89
SGPT
Result
Unit
Reference Ranges
L/N/H
Clinical Significance
84.0
U/L
30.0-65.0
H
An increase in SGPT level is due to impaired liver function caused by liver cirrhosis. It can be
ALT (SGPT) is, by caused by hepatic inflammation (including contrast, normally found infectious mononucleosis, pancreatitis, alcohol, largely in the liver. This viral hepatitis) is not to say that it is exclusively located in liver but that is where it is most concentrated. It is released into the bloodstream as the result of liver injury. It therefore serves as a fairly specific indicator of liver status. SGOT
182.0
U/L
15.0-37.0
H
An increase in SGPT level is due to impaired liver function caused by liver cirrhosis. It can be
AST (SGOT) is normally
caused by hepatic inflammation (including
found in a diversity of
infectious mononucleosis, pancreatitis, alcohol,
tissues including liver,
viral hepatitis)
heart, muscle, kidney, and brain. It is released
90
91
DRUG STUDY
Deneric Name
Brand Name Classification
Furosemide Furoside, Lasix Myrosemide, Uritol, Diumide-K® (functional) Loop diuretic
(chemical) Sulfonamide derivative Dosage and Route 40 mg tab OD Mechanism of Inhibits reabsorption of sodium and chloride at proximal and distal tubule Action and in the loop of Henle Indication Pulmonary edema, hypertension, third spacing Contraindication Hypersensitivity to sulfonamides, anuria, hypovolemia, infants, lactation and electrolyte depletion Drug Interaction >increased toxicity with lithium, non-depolarizing skeletal muscle relaxant >increased hypotensive action with antihypertensives and nitrates Side/Adverse Effects
>increased ototoxicity with aminoglycosides, cisplatin, vancomycin CNS: headache, fatigue, weakness, vertigo CV: orthostatic hypotension, chest pain, ECG changes circulatory collapse EENT: loss of hearing, ear pain, tinnitus and blurred vision ELECT: hypokalemia, hypochloremic alkalosis, hypocalcemia, matabolic alkalosis
GI: nausea, diarrhea, dry mouth, abdominal cramps, gastric irritaions GU: polyuria, renal failure, glycosuria HEMA: thrombocytopenia, agranulocytosis, anemia Nursing
INTEG: rash, pruritus, purpura, diaphoresis >assess for drowsiness and restlessness for it may indicate metabolic
Responsibilities alkalosis >monitor for signs of hypokalemia; postural hypotension, malaise, fatigue, tachycardia, leg cramps and weakness >observe hearing problems including tinnitus and hearing loss >monitor I & O qd to determine fluid loss. >monitor vital signs; rate, depth, and rhythm of respiration >ister in AM to avoid interference with sleep if using drug as diuretic > Use sterile equipment and apply principles of asepsis. > Ensure correct identification of the patient prior to the procedure. >Decontaminate hands prior to the procedure. >The cannula insertion site should be inspected for complications, i.e. infiltration, infection. >instruct patient to increase fluid intake 2-3 L/day unless contraindicated >tell the patient to rise slowly from lying or sitting position because orthostatic hypotension may occur >evaluate for therapeutic response
Generic Name Brand Name Photo
Omeprazole Losec and Prilosec
Classification Gastric acid secretion, proton-pump inhibitor Dosage and Route 40mg IVTTq12 Mechanism of Suppress gastric acid secretion by inhibiting the partial cell H+/K+ Action Indication Contraindication Drug Interaction
ATP pump To prevent ulceration in patients under NPO Known hypersensitivity to omeprazole decreased effect: decreased ketoconazole; decreased itriconazole increased toxicity: diazepam increase half-life; increased digoxin,
increased phenytoin, increased warfarin Side/Adverse EffectsCNS: headache, dizziness Neuromascular & Skeletal: weakness, back pain GI: nausea, diarrhea, vomiting, abdominal pain, constipation, taste perversion Nursing Responsibilities
Respiratory: upper respiratory infection, cough Ensure ten rights of medication istration Instruct patient not to chew, crush or open capsule Instruct patient to take before eating, capsule should be swallowed whole
Warn patients that Zegerid contains 460 mg sodium bicarbonate per dose. Those following a sodium-restricted diet should be cautious. Tell patient to empty contents of Zegerid packet into a small cup containing 2 tablespoons of water. Instruct patient to take drugs 30 minutes before meals. Caution patient to avoid hazardous activities if he gets dizzy. Inform patient that prilosec OTC may take 1-4 days for full effect.
Generic Name Brand Name Photo Classification
Spironolactone Aldactone Electrolyte and water balance agent; potassium sparing diuretic
Dosage and Route PO – (25, 50, 100) mg tablets
DOSING: Edema – 25 – 200 mg/d in divided doses, continued for atleast 5 daysd
Mechanism of
One of the main functions of the kidneys is to retain salt (sodium
Action
chloride) and water in the body. In patients with heart failure and cirrhosis, increased levels of a hormone produced by the adrenal glands, called aldosterone, causes salt and fluid to be retained by the kidneys. (At the same time, it also causes the kidneys to eliminate potassium.) The body becomes overloaded with salt and water, and this worsens the heart failure. Spironolactone inhibits the action of aldosterone thereby causing the kidneys to excrete salt and fluid in the urine while retaining potassium. Therefore, spironolactone is classified as a potassium-sparing diuretic, a drug that promotes the output of urine (diuretic) while allowing the kidneys to hold onto
Indication
potassium. clinical conditions associated with augmented aldosterone production, as in essential hypertension, refractory edema due to CHF, hepatic cirrhosis, nephritic syndrome and idiopathic edema
Contraindication Patients
with
anuria,
acute
renal
insufficiency,
significant
impairment of renal excretory function, or hyperkalemia. Drug Interaction Spironolactone can lower blood sodium levels while raising blood potassium levels. Excessively high blood potassium levels can lead to potentially life-threatening abnormalities in the rhythm of the heart. Therefore, spironolactone usually is not istered with
Generic Name
Ceftriaxone
Photo
Brand Name
Rocephin
Classification
cephalosporin antibiotic
Dosage and Route
1gm IVTTq12
Mechanism of
This antimicrobial agent inhibits bacterial cell wall synthesis by
Action
binding to one or more of the penicillin-binding proteins (PBPs) which in turn inhibits the final transpeptidation step of peptidoglycan synthesis in bacterial cell walls, thus inhibiting cell wall biosynthesis. Bacteria eventually lyse due to ongoing activity of cell wall autolytic enzymes (autolysins and murein hydrolases) while cell wall assembly is arrested.
Indication
Respiratory tract and intraabdominal infections
Contraindication
Cephalosporin hypersensitivity.
Drug Interaction
Warfarin (Coumadin, Jantoven) If you are taking ceftriaxone and warfarin, your body may metabolize the drugs differently than intended. You healthcare provider may choose to monitor your INR and prothrombin time more frequently and adjust accordingly. INR and prothrombin time are tests used to measure how well your blood clots.
Probenecid (Benemid, Probalan) If you are taking both ceftriaxone and probenecid, your body may metabolize the drugs differently than intended and significantly increase the amount of ceftriaxone in your system. Your healthcare provider may choose to monitor your progress
Generic Name
metronidazole
Photo
Brand Name
Flagyl
Classification
Anti-infectives, antiprotozoals, antiulcer agents
Dosage and Route Mechanism of Action
500mg 1 TAB q6 Disrupts DNA and protein synthesis susceptible organisms. Therapeutic effects: Bactericidal, trichomonacidal or amebicidal action. Spectrum: Most notable for activity against anaerobic bacteria including: Bacteroides, clostridium. In addition is active against: Trichomonas vaginalis, entamoeba histolytica, giardia lamdia, H. pylori and clostridium difficile.
Indication
PO: Amebecide in the management of amebic dysentery, amebic liver abscess and trichomoniasis: treatment of peptic ulcer disease caused by Helicobacter pylori.
Contraindication
Hypersensitivity. Use cautiously in: history in blood dyscrasias, History of seizures or neurologic problems and severe hepatic impairement.
Drug Interaction
Drug-drug: Cimetidine may decrease metabolism of metronidazole. Phenobarbital and rifampin increases metabolism and may decrease effectiveness. Metronidazole increases the effects of phenytoin, lithium, and warfarin. Disulfiram-like reaction may occur with alcohol ingestion. May cause acute psychosis and confusion with disulfiram. Increased risk of leucopenia with fluorourousel or azathioprine.
Side/Adverse Effects CNS: Seizures, dizziness, headache.
Generic Name
Lactulose
Photo
Brand Name
Contulose
Classification
Laxative
Dosage and Route
30cc @ bedtime
Mechanism of
Produces osmotic effect in colon. Resulting distention promotes
Action
peristalsis. Decrease blood ammonia build- up the causes hepatic encephalopathy, probably ass result of bacterial degradation which lowers pH of colon contents. Relieves constipation, decreases ammonia concentration.
Indication
- constipation - To prevent and treat hepatic encephalopathy, including hepatic precoma and coma I patients with severe hepatic disease. - to restore bowel movements after hemorrhoidectomy.
Contraindication
Contraindicated in patients on low- galactose diet
Drug Interaction
Drug-drug. - Should not be used with other laxatives in the treatment of hepatic encephalopathy - Anti- infectives may diminish effectiveness in treatment of hepatic encephalopathy
Side/Adverse Effects GI: belching, cramps, distention, flatulence, diarrhea ENDO: Hyperglycemia Nursing
Generic Name
Essentiale Forte
Photo
Brand Name
Essential Forte
Classification
Cholagogues, Cholelitholytics & Hepatic Protectors
Dosage and Route
1 cap TID
Mechanism of
Increase functional status of the liver, improvement in the lipids
Action
metabolism caused by accelerated synthesis of lipoproteins in the liver, activation of the phospholipid-depending ferments, increased synthesis of glycogen in the liver, decreased the fatty infiltration of the hepatocytes
Indication
- cirrhosis - Hepatic steatosis (also in cases of diabetes) - Acute and chronic hepatitis - Necrosis of the liver cells - Hepatic coma and precoma - Toxic liver damage (including pregnancy toxicosis)
Contraindication
- Contraindicated in patients hypersensitive to drug -in newborn children -in pregnant women
Drug Interaction
Not indicated
Side/Adverse Effects In very rare cases it can cause :abdominal pain, nausea, diarrhea and allergic reaction(skin rash). Nursing Responsibilities
1. Instruct patient on proper use of the drug
Generic Name
Phytonadione
Photo
Brand Name
Aqua-Mephyton, Vitamin K
Classification
Vitamin ( fat soluble)
Dosage and Route Mechanism of Action
1 amp now, OD -Required for hepatic synthesis of blood coagulation factors II (prothrombin), VII, IX, and X. - prevention of bleeding due to hypoprothrombinemia
Indication
•
Anticoagulant-induced prothrombin deficiency caused by coumarin or indanedione derivatives;
•
Prophylaxis and therapy of hemorrhagic disease of the newborn;
•
hypoprothrombinemia due to anti-bacterial therapy;
•
hypoprothrombinemia secondary to factors limiting absorption or synthesis of vitamin K, e.g., obstructive jaundice, biliary fistula, sprue, ulcerative coilitis, celiac disease, intestinal resection, cystic fibrosis of the pancreas, and regional enteritis;
•
Contraindication Drug Interaction
other drug-induced hypoprothrombinemia.
Hypersensitivity to any component of this medication. -Large doses will counteract the effect of warfarin - large doses of salicylates or broad-spectrum
Generic name
paracetamol
Photo
Brand name
Aeknin
Classification
Therapeutic: antipyretics, non-opiod analgesics
Ordered Dosage and
300mg IVTT now
Frequency Mode of Action
Inhibits the synthesis of prostaglandins that may serve as mediators of pain and fever, primarily in the CNS. Has no a significant anti-inflammatory property or GI toxicity. Therapeutic Effects: analgesia, antipyresis.
Indication
Mild pain, Fever
Contraindication
Contraindicated in: Previous hypersensitivity. Products containing alcohol, aspartame, saccharin, sugar, or tartrazine should be avoided in patients who have hypersensitivity or intolerance to these compounds. Used cautiously in: Hepatic disease/renal disease; chronic alcohol use/abuse; Malnutrition
Drug Interactions
Drug-drug: Chronic high-dose acetaminophen may increase the risk of bleeding with warfarin. Hepatoxicity is additive with other hapatotoxic substances, including alcohol.
Adverse Reactions/ Side Effects
GI: Hepatic failure, hepatoxicity (overdose) GU: renal failure(high doses/chronic use) Hemat: neutropenia, pancytopenia, leukopenia
Generic name
Tranexemic acid
Photo
Brand name
Cyclokapron
Classification
Hemostatic agent, antifibronolytic agent
Ordered Dosage and
100mg IVTT q8
Frequency Mode of Action
Inhibits activation of plasminogen, thereby preventing the conversion of plasminogen to plasmin
Indication
Prevention of hemorrhage
Contraindication
Hypersensitivity, active intravascular clotting
Drug Interactions
Concurrent use of clotting factor, complexes may increase the risk of thrombotic complications. risk of thrombosis may be increased by estrogens. Drug will antagonize the effects of thrombolytic agents.
Adverse Reactions/ Side Effects
CNS: visual abnormalities CV: hypotension, thrombosis, thromboembolism GI: nausea, vomiting, diarrhea
Nursing
i.
Responsibilities
observe the 10 rights of medication istration of medication
ii.
check for hypersensitivity to drug
iii.
observe for bleeding
iv.
instruct patient ot take tranexamic acid as directed
NURSING THEORIES
Theorist: Dorothea Orem Theory: Self-care Deficit Theory Orem’s theory states that each person has a need for self care in order to maintain optimal health and wellness. Each person possesses the ability and responsibility to care for themselves and dependants. The theory is separated into three conceptual theories which include: self-care, self-care deficit, and nursing system. Self care is the ability to perform activities and meet personal needs with the goal of maintaining health and wellness of mind, body and spirit. Self-care is a learned behavior influenced by the metaparadigm of person, environment, health and nursing. There are three components of this theory: universal self-care needs, developmental self-care needs, and health deviation. Universal theory includes activities which are essential to health and vitality. Developmental self-care need include the interventions and teachings designed to return to a person to or sustain a level of optimal health and well-being. Health Deviation selfcare encomes the variation of meeting self-care which may occur as a result of disability, illness or injury. Orem created three areas of how care can be istrated to a client depending on the physical and mental capabilities of the client: the wholly compensatory, partly compensatory and the ive-educative role. The wholly compensatory system accomplishes the client’s therapeutic self-care, compensates for the client’s inability to participate in their self-care, provides and protects the client. The partly compensatory is a give and take system between the client and the nurse. The nurse performs, compensates and assists the client as needed while the client participates,
regulates and accepts care and assistance form the nurse. Lastly, the ive-educative role indicates that the client is participating in most of their self-care, and the nurse’s role is simply to monitor and regulate the client’s self-care.
Application to client: The client’s environment failed to provide adequate warmth and ventilation. It has a limited space and is not quiet enough for the client to take adequate rest. These factors contributed to the client’s present condition as well as his ability to cope and recover. The nurse’s role is to help client achieve optimal health and wellness by acting as an advocate, redirector, person and teacher and to provide an environment conducive to therapeutic development. One example of this theory is by creating nursing care plans which was made by the student nurses. The theory applies to the assessment and evaluation of the nursing process. Since patient is in a comatose state, we have applied the wholly compensatory system. Since patient is unable to do the self-care activities, the nurse together with the medical team assisted the client’s needs by providing adequate care to the patient through helping the client achieve good hygiene, preventing bed sore by turning the patient to sides, preventing injury and promoting rest and comfort to the patient. Also, nurses were able to create nursing care plans which became their guide on how to render care to the patient. Also, important health teachings were provided to the family of the patient.
Theorist: Lydia Hall Theory: Core, Care and Cure Theory Hall's theory emphasizes the importance of individuals as unique, capable of growth and learning, and requiring a total person approach. Her definition of health can be inferred to a state of self-awareness with conscious selection of behaviors that are optimal for that individual. Hall stresses the need to help the person explore the meaning of his or her behavior to identify and overcome problems through developing self-identity and maturity. The concept of society or environment is dealt with in relation to the individual. Hall's theory of nursing involves three interlocking circles, each one of it represents one aspect of nursing. The same aspect represents intimate bodily care of the patient. The core aspect deals with the innermost feeling and motivations of the patient and family through the medical aspects of care. Care is the sole function of nurses, where as core and cure are shared with other of the health care team. The major purpose of care is to achieve interpersonal relationship with the individual. The nurse plans and prepares a series of independent nursing interventions that can aid from its condition. These interventions are designed to provide good and conducive atmosphere, istering drugs to the right patient, right drug and right time. The nurse also provides health teachings to the client’s family on medication management and independent actions such as advising the client to have complete bed rest.
Theorist: Faye Glenn Abdellah Theory: Twenty-one Nusring Problems Abdellah’s theory would state that nursing is the use of the problem solving approach with key nursing problems related to health needs of people. Such a statement maintains problem solving as the vehicle for the nursing problems as the client is moved toward health – the outcome. Faye Abdellah formulated the twenty-one Nursing Problems and categorizes them into three: the Physical, sociological, and emotional needs of clients, the types of interpersonal relationships between the nurse and patient and the common elements of client care. The 21 Nursing Problems were divided into four care needs: Basic to all patients, Sustenal care needs, Remedial care needs and Restorative care needs. The Nursing problem presented by a client is a condition faced by the client or client’s family that the nurse through the performance of professional functions can assist them to meet. An overt nursing problem is an apparent condition faced by the patient or family, which the nurse can assist him or them to meet through the performance of her professional functions. The covert nursing problem is a concealed or hidden condition faced, by the patient or family, which the nurse can assist him or them to meet through
the performance of her professional functions. According to Abdellah, nursing is a helping profession.
Application to Client: Since our patient is suffering from his condition, the student nurses have identified nursing problems which made them choose the theory of Abdellah. The patient was in a state of coma and so he was not able to perform certain activities which he needs. Thus, student nurses provided care and assisted the client and his family. Some of the nursing interventions done to address the problems identified by the student nurses which falls under the 21 nursing problems theory were: maintained good hygiene and physical comfort, promoted rest and sleep, promoted safety through the prevention of accidents, injury, or other trauma and through the prevention of the spread of infection, maintained good body mechanics and prevent and correct deformity, To facilitate the maintenance of a supply of oxygen to all body cells, facilitated the maintenance of elimination, recognize the physiological responses of the body to disease conditions, created and / or maintained a therapeutic environment. The student nurses focused their interventions to the needs of the patient which helps in the promotion of recovery to the patient.
NURSING CARE PLANS Date / Time
Cues
February
Objective:
A
- crackles
C
11, 2010 at 4pm
heard on lung field upon ausculatation -with bag valve connected to endotracheal tube
Needs
T I
Nursing Diagnosis
Ineffective airway
At the end of
clearance related to
7 hours span
accumulation of
of care, the
secretions secondary
patient will
to Community
have
Acquired Pneumonia
effective
V I T Y E X E
Objective of Care
airway as evidenced by R: Pneumonia, which
absence of
is an acute infection
crackles.
of the lungs, causes inflammation in lung tissues which leads to
Nursing Intervention
1. Provide suctioning. R: to clear airway from accumulated
Evaluation
February 11, 2010; 11pm
secretions.
GOAL UNMET
2. Elevate head of bed.
After rendering
R: Gravity decreases pressure on the diaphragm 3. Turn patient to sides every 2 hours R: repositiong enhances drainage and promotes ventilation to different lung segments.
nursing interventions within the 7hours span of care, the patient has still ineffective airway clearance
damage on mucous
4. Assist in providing respiratory
as evidenced by
and alveolar
through ambu bagging.
presence of
membranes. This damage results in secretion of exudates and mucous as the
R: mechanical ventilation maintains adequate airways and improve respiratory functions.
crackles on lung field.
R C I S
system tries to get rid with the infection. This secretions cause obstruction in the airway.
A T T E R N
R: to maintain anatomic position of the tongue and provide natural airway 6. Re-ausculate lung sound R: to note for progress, if crackles are
E P
5. Insert mouth guard.
Williams, L.S &
still present.
Hoppers, P.D. (2007).
7. Provide oxygen with appropriate
Understanding
humidifier, as ordered.
medical-surgical nursing,3rd ed. Philadelphia: F.A. Davis Company.
R: to facilitate oxygenation and liquefy secretion for easy suctioning. 8. Monitor oxygen saturation. R: to rule out presence of gas exchange impairement. 9. Carry out diagnostic orders made by the physician such as ABG or AFB and secure result. R: to determine the degree of respiratory impairment such as
presence of hypoxemia.
Date
Cues
Needs
Nursing. Diagnosis
F
Objective cues:
N
Bleeding related to altered
E B R
-
Melena
noted Decreas
U
-
A
ed platelet
R
count of 115
Y
x103 /uL (Normal:
11,
150-400
2010
x103 /uL)
@ 5:00 PM
-
Gastric
lavage ordered
U T R I T I O N A L
Intervention
Evaluation
Within the 8
1. Monitor patient’s vital
February 11, 2010
clotting mechanism:
hours span of
signs, especially the
decreased prothrombin and
care, the patient
blood pressure
thrombin production
will be able to:
secondary to liver cirrhosis
M E
® To obtain baseline
maintain normal
data and prevent
® One of the functions of
hemodynamic
hypotension
liver is the production of
status as
prothrombin and thrombin
evidenced by a
which are substances
normal intake
needed to help blood
and output
2. Assess patient’s level of consciousness ® A change in the level
coagulate. In patients with
of consciousness
liver cirrhosis, they are at
indicates a decrease in
higher instances of
circulating blood volume
bleeding because of the decreased coagulation factors.
-
Objective
3. Monitor intake and output ® To determine fluid balance and prevent dehydration 4. Regulate intravenous
T
fluids appropriately
A
® To prevent
B
dehydration and correct the normal
O
hemodynamic status
L
5. Monitor hematocrit and
@ 10:30 PM Goal Met Within the 8 hours span of care, the patient was able to maintain normal hemodynamic status as evidenced by a normal intake and output
Date /Time February
Cues Objective Cue:
Nursing Diagnosis
Objective/Goal
Intervention
N
Hyperthermia related to the
Within my 1-3 hour
1.
U
release of endogenous
span of care, my
signs.
- Increased
T
pyrogen secondary to
patient’s body
® serves as baseline data
body
R
presence of CAP and liver
temperature will
temperature of
I
cirrhosis
decrease from 38.1°C
2.
38.3
T
to 36.5-37.5°C.
developmental age of client.
11, 2010 5:00pm
Needs
Monitor patient’s vital
@ Note chronological and
R: Hyperthermia is the
® Elderly or impaired
O
elevation of body temperature
individuals ay not be able to
is warm to
N
above normal range. Most
recognize and/or act on
touch
A
often, it results from infection
symptoms of hyperthermia
L
somewhere i the body, but it
-
Skin
Increa
sed
diagnos
is of CAP
GOAL MET Patient’s body temperature
3.
conditions (cancer, allergic
bath
from 38.1 ° C
reactions, and CNS injuries).
® promotes heat loss by
to 36.7° C
M
Macrophages, white blood
evaporation and conduction
E
cells, and injured cells release
T
chemical substances called
4.
A
pyrogens that act directly on
lightweight, loose-fitting
B
the hypothalamus, causing its
clothes.
O
thermostat to be set to a
® encourages heat loss by
respiratory
-
8:00pm
may be caused by other -
rate of 24
February 11, 2010
I -
Evaluation
Provide tepid sponge
Limit clothing in
decreased
-
ascites
L
higher temperature.
radiation and conduction.
Reference:
5.
Nurse’s Pocket Guide 10th
with air-conditioning or fans.
Edition by Doenges, et al.
® promotes heat loss by
I C P A
Cool the environment
convection
T T
6.
Keep clothing and linens
E
dry.
R
® to reduce shivering
N 7.
ister replacement
fluids and electrolytes ® to replace fluids lost through perspiration and respiration. 8.
Maintain bedrest
® to reduce metabolic demands 9. Discuss importance of adequate fluid intake
® To prevent dehydration INTERDEPENDENT 10.
Collaborate with
dietician in providing patient with high-calorie diet, or parenteral nutrition ® to meet increased metabolic demands 11.
Notify physician if
pharmacologic regimen is inadequate to meet hyperthermia control goal. ® to determine if there is a need to increase dosage, change medication or use a stepped program (e.g., switching from injection to oral route, or lengthening time interval between doses).
DEPENDENT 12.
ister antipyretics,
orally or rectally, as ordered. ® to aid in reducing the body temperature 13.
Provide supplemental
oxygen as ordered. ® to offset increased oxygen demands and consumption. 14.
ister replacement
IV fluids and electrolytes as ordered. ® to circulating volume and tissue perfusion and to aid in hydration
DATE/ CUES
NEE
NURSING
OBJECTIVES OF
D
DIAGNOSIS
CARE
TIME F
Objective:
E B R U A
N - ascites -dry, scaly and shiny -edema
R Y
U T R I T
-dyspnea
I O
1
N
1
A
,
L -
Fluid
Within 8 hours span
Volume
of care, the client
Excess in the
will be able to :
NURSING INTERVENTIONS
1.
® To obtain baseline date and
space related to liver organ
a. Stabilize
failure as
fluid volume as
evidenced by
evidenced by
2.
ascites
balanced I/O,
dependent venous pooling or
with liver failure, there is a decreased
Vital signs within normal limits
venostasis. ® To determine causative factors 3.
Thus,
environment, limiting external
osmotic
Provide quiet
stimuli. ® To promote adequate rest
2
M
pressure in
0
E
the
and comfort for faster
intravascular
recovery
1
T
spaces. This
0
A
leads to the
4.
Monitor intake and output
accumulation @
B
of fluid in the
Goal Unmet
Assess for evidence of
albumin.
decrease in
11:00 pm
to note any unusualities
production of
resulting to
February 11, 2010
Measure vital signs
@
interstitial
®In patients
EVALUATION
® To determine elimination o
Patient was unable to: o
stabilize fluid volume as evidenced by imbalance intake and output
Date / Time
Cues
February
Objective:
N
-
U
11, 2010 at
Needs
Nursing Diagnosis w/ Rationale
4pm
Jaundice noted in the skin upon inspection .
-
+4 pitting edema noted on all four extremitie
T R I T I O N
s -
(+) body malaise
A
Risk for impaired
Within my
skin integrity related
seven hours
to prolonged bed rest
span of care,
R: When edema and jaundice are present, the skin is placed at more risk of being
the patient will maintain undamaged physical
impaired because of
Skin integrity
the bilirubin present
by not
on the blood.
manifesting
Moreover, prolonged bed rest can form decubitus ulcers at the patient’s back.
L
Vital Signs: BP- 110/70
Objective of Care
signs of decubitus ulcer.
Nursing Intervention w/ Rationale 1. Monitor patient’s vital signs. ® serves as baseline data
February 11, 2010; 10pm
2.) Assess for any changes in skin. ® to be able to determine the causative factors 3.) Note and record degree of jaundice of skin and sclera and scratches on the body. ® to be able to assess skin integrity 4.) Maintain strict skin hygiene.
Goal Met: After seven hours span of care, the patient still maintained intact skin integrity as evidenced by absence of
® to prevent the spread of bacteria
decubitus ulcer
and prevent infection
at the patient’s
5.) Provide adequate clothing/covers. Reference :
Evaluation
®to prevent vasoconstriction
back.
mmHg
M
PR- 96 bpm
E
RR- 24 cycles
T
per minute TEMP. – 38.3 °C
Nurse’s Pocket Guide
6.) Observe for reddened/blanched
11th Edition by
areas and institute treatment
Doenges, et al.
immediately. ®: Reduces likelihood of progression
A
to skin breakdown.
B
7.) Change patient’s position every
O L I C
two hours. ®: To relieve the pressure on the patient’s back. 8.) Drain urine bag every two hours. To monitor output of patient in order to determine fluid and electrolyte
P A T T E
intake and loses 9.) Encourage frequent skin care to significant other. Also, perform morning care to patient by performing complete bed bath and apply lotion afterwards. ®: To promote hygiene and skin
R N
integrity. To promote skin moisture, and prevent roughness on skin. 10.) Emphasize importance of adequate nutritional/fluid intake to significant others. (through NGT feeding) ®: to maintain general good health and skin turgor. 11.) ister medications as ordered. ® to treat any underlying cause
POST-MORTEM
Ask permission to the family before doing the post-mortem care.
R: The family is in grieving stage and so nurses should be sensitive enough in dong responsibilities
Ask permission to the patient before removing tubing from his body
R: It is to convey respect and value to the patient’s body
Use caution when removing tape from the body to avoid skin breakdown.
R: The body temperature decreases with a resultant lack of skin elasticity
Elevate the head to prevent discoloration from the pooling of blood.
R: a physiological change will happen in which a bluish purple discoloration that is a by-product of red blood cell destruction occurs in the dependent areas in the body.
The nurse should close the eyelids, insert dentures, close the mouth and position the body in a natural position as soon as possible after death.
R: To prevent the body from stiffening caused by contraction of skeletal and smooth muscles.
Prepare the body: remove all tubes and position the body
R: To make the body look comfortable and natural for family viewing.
Place the body in a plastic or fabric shroud and put a tag on it.
R: To prepare the body for transport to the morgue.
Return the deceased’s possession to the family such as jewelries, eyeglasses, clothing and all personal items.
Offer to people
Help the family with decision making regarding funeral home, transportation, and the removal of the deceased’s belongings.
R: The family needs help since they are on the process of grieving.
Demonstrate comion in providing information and to families.
R: This will inform the family of your genuine concern for them
PROGNOSIS
Criteria Onset of Illness
Poor
Fair
Good
Justification We rated it poor since the
patient started manifesting symptoms that are associated with liver cirrhosis since December 2009. On January 23, 2010, 13 days prior to his ission, the patient experienced headache, chest pain, dull abdominal pain, felt nauseated and dizzy.. Duration of
Occurrence of
Illness
manifestations related to liver cirrhosis has been observed to start since December 2009. It is also poor since liver cirrhosis is a chronic disease. Hospital days until our last with the patient are 6 days.
Attitude and
As verbalized by his wife,
willingness to
the patient is taking
take
medications but sometimes
medications
with skipped doses because he neglects to take and due to forgetfulness.
Age
The patient is 73 years old and we rated it as poor since geriatric patients have deteriorating body systems that hinder recovery. The wear and tear theory suggests that as a person ages, he or she is more prone to illness and resistance and the ability to heal is getting weaker.
Precipitating
We rated it poor since his
and
age and race predisposes
predisposing
him in developing the
factors
disease. Moreover, his chronic alcoholism precipitates the development of the disease. Longtime alcohol beverage drinking is
the most common factor that triggers liver cirrhosis. Environment
The ward has poor
ventilation, crowded and noisy. With this, it is not favorable for recovery. Family
Family is fair. They give time in giving care to the patient but cannot provide all the needs especially the medications and mechanical ventilator because of financial inadequacy.
Basis for Prognosis: Poor = 1
Fair = 2
Good = 3
Range of prognosis: 0-1.50 = poor 1.51-2.0 = fair 2.0-2.5 = good
Result: POOR: Precipitating and predisposing factors, Age, Duration of Illness, Onset of Illness, Environment FAIR: Attitude and willingness to take medications and Family GOOD: None
Computation: Good: 3 x 0 = 0 Fair: 2 x 2 = 4 Poor: 1 x 5 = 5 Total: 9/7 = 1.28 (POOR PROGNOSIS)
RECOMMENDATION Every rotation we have is a learning course and practice to develop our skills and hearts as caregivers. In this rotation, the 3rd group of BSN-3H, cultured a lot of knowledge in this experience; experience that will serve as our guide and basis for improvement. In relation with improvement, the group had come up with recommendations, which we think, would have made the exposure a lot better. To our client’s family: One of the most important factors of recovery for a certain illness is the participation of the patient himself. However, our client has suffered a disease wherein he has gone seriously affected both physically and emotionally and even his consciousness and responsiveness have been depleted. The family’s involvement in the treatment of the patient is very essential and highly needed. The family should know all the basic facts and information about the patient’s illness because them, more than anybody else are expected not just to care but also to accept his condition with utmost understanding. Being aware of the illness itself and its treatment will elicit awareness and would definitely pave the way to the prevention and alleviation of any ailment that any of the family may possibly have. To the family , the death of a love one is not the end of every one’s life. His death should serve a lesson and be a step towards taking good care of one’s body.
To the Student Nurses: In line with this case study, the group would like to encourage all student nurses to get more involved in the promotion of health in our country. We are to provide health services to the greater population in a way that it is more generalized. We must impart to those who are in need, our knowledge regarding health and on how they could maintain a healthy lifestyle. We must apply to them the skills that we have learned by rendering them a quality- based service. We must also teach the patients as well as the significant others on the alternative means of promoting health and on how to prevent the possible occurrence of a disease. Empathy must always be shown not just to the patient but also to the significant others. Student nurses must also be sensitive to the feelings and emotions not just of the patient but also to the significant others especially in experiences of death and finite separation. To the medical world:
We would like to encourage the medical practitioners or the of the health care team that they should have to be more committed or comionate in their chosen profession. They must have to cater the health needs of the people of different kinds without putting levels of discrimination on them. Their job is not that easy but they must have to be very careful because they are already dealing here with the life of a person. They must have to extend their hands not only in the physical means but also in a holistic way of giving or providing care to individuals, families and the population groups especially in significant others who may have lost love ones.. They are tasked to render
their services in order to achieve the good health condition of the citizens of the country because the health of the nation lies in the health of the populace.
REFERENCES
BLACKWELL’S DICTIONARY OF NURSING 5TH EDITION, 2004 BROWN, K.S (2003) DEVELOPMENTAL THEORY: UNDERSTANDING THE AGES. RETRIEVED FROM HTTP://WWW.HAVERFORD.EDU/PSYCH/DDAVIS/P109G ERIKSON.STAGES.HTML. RETRIEVED ON FEBRUARY
12, 2010.
HANDBOOK OF MEDICAL-SURGICAL NURSING 3RD ED. SPRINGHOUSE: 2006 LEIGHTON, S.S., ET AL.(1997) PERSPECTIVE IN HUMAN DEVELOPMENT. RETRIEVED FROM HTTP://WWW.SLIDESHARE.NET/SUNNYCUTS/JEAN-PIAGETS-THEORIES-OF-DEVELOPMENT. RETRIEVED ON FEBRUARY 20, 2010. LINDON, P.S & REESE, R.R. ( 1999) PSYCHOLOGY: APPROACH AND UNDERSTANDING. RETRIEVED FROM HTTP://PSYCHOLOGY.ABOUT.COM/OD/THEORIESOFPERSONA LITY /A/PSYCHOSOCIAL_3 .HTM. RETRIEVED ON
FEBRUARY 12, 2010.
LINDON, P.S & REESE, R.R. ( 1999) PSYCHOLOGY: APPROACH AND UNDERSTANDING. RETRIEVED FROM HTTP://EDUCATION.STATEUNIVERSITY.COM/PAGES/2032/HAVIGHURST-ROBERT-J-19001991.HTML. RETRIEVED ON FEBRUARY 12, 2010. LUCKMANN, K.L & SORENSEN, W.A (2003) : MEDICAL-SURGICAL NURSING: A PSYCHOPHYSIOLOGIC APPROACH. LOUIS, MISSOURI: MOSBY. MCTIMOTHY, A.S (2005) PATHOPHYSIOLOGY: A 2-IN-1 REFERENCE FOR NURSES. PHILADELPHIA: LIPPINCOTT WILLIAMS & WILKINS. PETERSON, M.L, LUIS, B.D. & CHONG, P.C.(2000)PERSONALITY DEVELOPMENT. RETRIEVED FROM HTTP://BAMA.UA.EDU/~JSTALLWO/YAL/ARTICLES/YOUNG%20ADULT%20LITERATURE%20IN %2 0THE%20CLASSROOM.PDF. RETRIEVED ON FEBRUARY 22, 2010.
REYBURN, S. W. (2001) MANUAL OF MEDICAL EDUCATION. RETRIEVEDFROM HTTP://WWW .AAFP.ORG/AFP /2006/0201/P44 2.HTML ACCESSED ON FEBRUARY 21, 2010 SUDDARTH, D.R. (1991) THE LIPPINCOTT MANUAL OF NURSING PRACTICE, 5TH ED. PHILADELPHIA: LIPPINCOTT WILLIAMS & WILKINS. WONG, L.D. (2000) UNDERSTANDING LIVER CIRRHOSIS. RETRIEVED FROM HTTP://WWW.EMEDICINEHEALTH.COM/CIRRHOSIS/PAGE2_EM.HTM#CIRRHOSIS%20CAUSES.
RETRIEVED ON FEBRUARY 22, 2010.
The group would like to express their heartfelt gratitude, sincere appreciation and profound regards to the following people who, in one way or another, gave guidance, strength, and encouragement in making this case presentation possible. First of all, to Almighty God the Father, who granted us the knowledge and skills, Who send forth the gift of Holy spirit that aided them in completing this study. Without Him, none of these things would be possible. To their family, friends, and classmates, for their consideration and unending , emotionally, spiritually and financially. To their clinical instructor, Mrs. Jocelyn Ferraren, RN, for guiding us in the course of making this case presentation and giving them tips on how to have a good presentation. To all medical personnel and staff of DMC, MED- ward, for the warm accommodation during their clinical exposure and for giving them inspiration to keep the spirit of caring burning. To the of the group, for sharing ideas, cooperating and giving full effort in making the case presentation successful.
1
Lastly, to our client and his family for their acceptance and willingness to share time, effort and giving us the essential information needed for this case presentation.
INTRODUCTION The liver is one of the largest and most complex organs in the body. It stores vital energy and nutrients, manufactures proteins and enzymes necessary for good health, protects the body from disease, and breaks down (or metabolizes) and helps remove harmful toxins, like alcohol, from the body. It is one of the most important organs in the body since it has many significant functions. A lack or failure to provide proper care of it may lead to an abnormality or disorder. One of the severe forms that may happen is Liver Cirrhosis. Liver Cirrhosis is derived from Greek word kirrhos, meaning "tawny" (the orange-yellow colour of the diseased liver).It is a chronic disease that causes cell destruction and fibrosis (scarring) of hepatic tissue. Fibrosis alters normal liver structure and vasculature, impairing blood and lymph flow and resulting in hepatic insufficiency and hypertension in the portal vein. Cirrhosis is most commonly caused by alcoholism, hepatitis B and C and fatty liver disease but has many other possible causes. Some cases are idiopathic, i.e., of unknown cause. It may be classified by the structural changes that take place or by the cause of the disorder. Internationally, liver cirrhosis is the 8thth most common cause of death. It is most common among people ages 45 – 75, killing more than 25,000 people each year, 50% of which are alcohol related. In the Philippines and other underdeveloped countries,
2
however, the incidence of liver cancer is rather high. Liver cancer is relatively common in our country primarily because many Filipinos suffer from cirrhosis of the liver, a major risk factor for liver cancer. Cirrhosis of the liver precedes 80 percent of all liver cancers; thus, any condition that predisposes to cirrhosis indirectly causes liver cancer. The usual cause of liver cirrhosis among Filipinos is chronic hepatitis B, a major public health problem in the country. Chronic hepatitis B afflicts between 10 and 12 percent of all Filipinos (i.e., more than 8 million Filipinos). Other less significant causes of cirrhosis are hepatitis C infection and alcoholism. The latest DOH advisory shows that liver cancer is the third most common form of cancer among Filipinos—in men, it is the second most common, while in women, it is the ninth most common. Locally, liver cirrhosis is the 17th leading cause of death here in Davao. In connection with it, last February 11, 2010, the Group 3 of section 3H was assigned on duty at the Davao Medical Center- Communicable Pavilion where they met their patient Mr. Cute who was diagnosed of having Liver Cirrhosis. They were motivated to learn more and study the disorder since it was their first time to encounter such case. Also, the group was more encouraged to choose the patient for their case presentation in order to acquire better understanding and to gain more knowledge and use it for the future.
3
OBJECTIVES To have a course of direction, organization and to recognize the essence of this study, we have set the following objectives:
GENERAL OBJECTIVES
After rendering effective nursing care for three days at the Davao Medical Center, MED- Ward, we aim: • To provide an extensive study about Community acquired pneumonia ascites
secondary to liver cirrhosis for us to gain better understanding about the disease and be equipped with competence in dealing with related situations in the future; • To improve our skills in doing relevant interventions which promote wellness to
persons having the disease; •
Not only to understand the situation of the client and their families who are confronted with the disease but also to empathize with them.
SPECIFIC OBJECTIVES
Find a case in the DMC, MED- ward within the three-day duty;
4
Establish a good interpersonal relationship with our chosen client as well as to his significant others;
Acquire necessary data of our client which are relevant to our case study;
Trace the patient’s family lineage and present remarkable familial disease;
Trace the health history of the client and the family by collecting information both from the past and present illnesses;
Evaluate the client’s development guided by Erik Erikson, Robert Havighurst and Jean Piaget’s Theory;
Define the complete diagnosis of our client guided by three different sources;
Perform cephalocaudal assessment to the client thoroughly;
Discuss the systems involved in the development of the disease in the human anatomy and physiology;
Present the etiology and symptomatology of the disease process with each of its rationales and identify which are present on the client’s case;
Trace the pathophysiology of the disease as experienced by our client and
Sends thesignal to the medulla oblongata to presentcough Crackles and Wheezes
it through a schematic diagram;
Present and analyze the doctor’s order in chronological manner;
Explain and interpret both actual and possible diagnostic studies including indication, result, and their implications;
The mucosal lining nerves detects the excessive the secretions
Exudates production and Edema Cilia try to propels the mucous out of the 5 system Stimulates mucous
large quantities
Discuss the different drugs taken by the patient with corresponding intervention;
Identify different nursing theories made by
Florence Nightingale,
Chemical mediators irritate the goblet cells of the bronchial nursing lining Stimulates Diapedesis and positive Virginia chemotaxis of Leukocytes
Henderson and Lydia Hall and relate it on the patient’s conditions;
Inflammation of the Parenchyma
Formulate specific, measurable, attainable, realistic, and time-bounded nursing care plans with corresponding rationales for each of the nursing interventions;
Evaluate the client’s progress with our continuous care; Render health teachings or appropriate nursing interventions necessary client and family as well;
Present a discharge plan for the patient
Fever
Obstruction of the airway
Cilia fail to sweep the mucous to the because of thickness Histamine causes vasodilation Prostaglandin and Leukotrienes causes blood vessels to be more permeable
Present and justify the prognosis of our patient
Provide recommendations for the better management of patient with the same disease in the future endeavor;
Accomplish our case presentation.
Damage of the cells release Histamine, Prostaglandins and Leukotrienes Blood vessels leak. Damage on the blood vessels is scant Predisposing factors: Age- elderly adults (age above 70)
Precipitating factors: Smoking Alcoholism
6 Hematemesis and
GI bleeding If treated: MGT: Transplantatio n Paracentesis Medications
PATIENT’S DATA
Name: Mr. Cutie Age: 72 years old Sex: Male Date of birth: May 23, 1937 Place of birth: Igacos, Davao City Current address: Manablay Callawa, Buhangin Davao City Occupation: Farmer Nationality: Filipino Religion: Christianity (Roman Catholic) Civil Status: Married
plasmaphorese s If not treated Progressive liver destruction, systemic counsel Hepatic encephalopath y Toxic substance production Mental retardation Hepatic coma
DEATH
Date of ission: February 6, 2010
- Destruction of cell membranes causes red blood cells to burst
Time of ission: 04:09PM
Nursing Resp:
CLINICAL DATA
Mode of ission: Ambulatory Chief complaint: malaise, loss of appetite, nausea, and black tarry stool
-Give supplements containing Vit.E
Nursing Resp: 7 -Give Vit.D fortified milk
-Give supplementati on
Ward: MED - itting physician: Dr. Emerson R. Taghoy Vital signs upon ission: Temp: 36.6 C BP: 90/60 mmHG PR: 65 bpm RR: 28 m Final diagnosis: CAP MR Ascites 2’ Liver Cirrhosis Source: Significant others and patient's chart
Varices and hemorrhoids May rupture and bleed Vitamin D Decrease absorption of calcium and Phosphorus from the GI tract Vitamin E Decrease against oxidative damage caused by free radicals Nursing Resp:
- Monitor urine output - Elevate edematous extremities -Reposition every 2 hours if patient - ister diuretics as prescribed - Tell patient to use antiembolic stockings or bandage 8 Nursing Resp: -Give
-prevent injury -decrease risk for infection
Development of tissues, and resistance to infections
GENOGRAM Lola-har
Lolo-har
Grandmade r
Body malaise
Titahar
PAPA-HAR
Manong
Decreased source of MAMA-HARenergy Auntie Decreased glucose in the body
Tito
Kol
Decreased vitamin K Gwaping
Boylet
Gwafa
Keks
Pefa A Vitamin
Cutie●
Vitamin deficiency Nursing Resp: -Encourage intake of Vit.K rich foods
LEGEND: MALE FEMALE
DECEASED TB HYPERTENSION ●
LIVER CIRRHOSIS
Nursing Resp: Nursing Resp: -Assess pain scale -Monitor VS -ister analgesic as ordered
9
Absence of bilirubin in the feces
FAMILY BACKGROUND AND HEALTH HISTORY Family History
Bile unable to reach Gi tract Clay colored stool ASCITES
Most of the significant details gathered on the interview we had came from
Third spacing occurs Mr.Cutie’s wife and daughter since he was not able to verbalize due to his condition. JAUNDICE
Upon the interview, we found out that no one in the family had any of the sickness that the patient had namely Liver Cirrhosis and Community Acquired Pneumonia.
Speeds up destruction of RBCs
Cutie is a married man with three children. He is the main decision maker in the
Chronic ive family as evidenced by his wife verbalizing,” siya man gyud ng gabuot ug unsay maayo congestion
para sa amoa”. In regards to their health, several of their family specifically the Spleen patient, his wife and his daughter have hypertension which was all diagnosed by GI the tract physician, whom they usually consult in Polyclinic Health Center where their neighbor Stomach pain works as a nurse. However they were not able to recall the name of the physicianAltered they bowel function
consulted, but they were able to the month and year that their condition was
Blood regurgitation diagnosed: on August of the year 2009. In reference to the diagnosis that was given by to the spleen , tract the physician, maintenance medication was given to the three of them howeverGIthey Prominent forgot since they only used the said the medication for about two weeks. Finances were a
distended factor since they were not able to comply the medication prescribed by the physician.blood vessels in the stomach Bleeding The family does not seek medical advice until the condition they have worsens as tendencies
stated by Cutie’s wife. All of them had experienced fever, flu, cough, colds, stomach
Shunting of pains, etc. but again they don’t seek medical attention until condition becomes worse.blood from portal vessels to vessels with lower pressure Decrease in osmotic pressure 10 KIDNEYS
Signal for aldosterone release
Lifestyle
Na+ absorption/ H2O retention
As verbalized by the patient’s wife, the patient at his young age was a typicalK+ excretion
adolescent who goes with friends and often explores things around. As stated, the patient
EDEMA
was curious at all things and because of that he was inclined to a number of vices which
No free blood age may actually have affected his health status. He was smoking badly as he was able to Backflow of bile
consume 1-2 packs of cigarette a day and drinks enormously as he was able to drink 1
long neck of Tanduay on his own. At times, he goes beyond 1 long neck and even drinks Bile goes to the blood
half a gallon of “Tuba” when he is not yet drunk. As stated by his wife, his husband doesstream
not stop drinking unless he becomes drunk. As the normal things go as stated by his Formation of collateral
wife, the patient and his drinking colleagues use same glass whenever they drink. All of vessels blood these had been the lifestyle of the client since then.
in the GI system Accumulation of ammonia
When he reached his adulthood, he worked as a farmer and still continued to
drink and smoke whenever he has time. He often sleeps at 10:00pm and wakes Unable up at to convert ammonia to urea
5:00am then takes his breakfast and goes to his work. He takes his break from 11:30am up to 12:30pm and thus eats his lunch. He goes to work and ends at 5:00pm. What he
Decreased
normally does is clean the plantation and get rid of unwanted growth of grasses allglucogenesis over the place that may alter the good growth of the trees that were present. Whenever he has Decrease in albumin
spare time such as weekends which is his rest day from work, he stays at home, watches production TV or talks with his children or goes to his neighbor and drinks. He had such routine Obstruction until of portal
last year, 2009, when he finally had stopped doing his usual things when he was circulation diagnosed of having hypertension. He drinks rarely and smokes only about 2-4 sticks aPortal day compared before when he was not yet diagnosed with hypertension.
hypertension Liver Decreased RBC 11 Body malaise, pallor
Change to Fowler’s position, assess CRT
Decreased erythropoietin
Diet
Hepatic fibrosis
The patient’s wife was able to notice that his husband was fond of eating fatty Impaired hepatocyte
foods such as “taba sa baboy.” Whenever they have this kind of viand, she reported that function
her husband would really eat a lot of these when available. She also mentioned that her changes Matrix husband liked eating salty foods such as dried fish and ginamos almost every day. It Extracellular has matrix
been said by the patient’s wife that these viands are the usual part of every meal.components In Predisposing addition to that, they often take canned goods. As the patient’s wife verbalized “Syempre Factors:
dong ana man gyud na sa pobre”. Moreover, drinking coffee every morning has always Male
been the routine of his husband, still reported by his wife.
Age (45-75 yrs old) Race
History of past illness Race: Asian
Other than ordinary fever, cough, and flu, which they treat only through over-thePathophysiology counter drugs and no consultations, the patient didn’t have any serious illness. This was of Liver Cirrhosis the case, however, until he reached the old age when different signs and symptoms started to manifest, increased blood pressure arise. He then sought medical advice since Precipitating factors:
there were other manifestations of hypertension such as dizziness, nausea and pain on his
nape. Then he found out that he has hypertension as diagnosed. Only through daily BP Chronic alcoholism
taking at Santo Tomas Clinic, a clinic just around the area, did they found out about this Diet
gradual increase in blood pressure. It was treated and taken cared of through unrecalled Smoking
medications that were prescribed to him by the said clinic. sMOK Portal obstruction Grandfader 12
History Of Present Illness For the past years, the patient did not have any serious illness related to his present condition. But on January 23, 2010, 2 weeks prior to the patient’s ission, he had headache, chest pain, dull abdominal pain, felt nauseated and dizzy. The patient and even his wife had never thought that it was a manifestation of an underlying problem and so they did not take it seriously. They did not seek medical attention; instead his wife gave him over-the-counter medication such as Paracetamol for his headache which he took four times during that day and one Diatabs for his stomach pain which is actually not appropriate since the medication itself was wrong and that the underlying condition was not taken into consideration. The condition however did not last long since it was relieved one day after it occurred. The patient and his wife were relieved and thought that it was just a “Panuhot and Kabuhi”. One week prior to patient’s ission to the hospital, his wife noticed that his husband had abdominal distention which she abruptly noticed as evidenced by her verbalization, “Dili man kaayo na siya dako ug tiyan sa una. Murag ning kalit ra man. Atong mga last week sa January ra pud nako nabantayan”. On the 2nd day of February, 2010, four days prior to ission to the hospital the patient sought consultation at the Emergency Room since the patient felt loss of appetite, stomach pain which radiated to the patient’s back and prandial vomiting. Despite the manifestations seen on the client, he was discharged and was requested to have an ultrasound of the abdomen. Aside from that, it was again diagnosed that he has hypertension so antihypertensive medications were prescribed. Days had gone and on the
13
6th of February 2010, the patient experienced body malaise, loss of appetite, nausea, and black tarry stool which were his chief complaint that resulted to his ission to Davao Medical Center.
14
DEVELOPMENTAL DATA
Erik Erikson’s Psychosocial Theory of Development Theory
Stage
Result and Justification
Erik Erikson, in his
Integrity versus Despair
The patient has fully
Psychosocial Theory of
(65 years old and above)
achieved integrity.
development, believed that
This stage focuses on
According to his wife,
personality develops in a
reflecting back on life.
Cutie is already contented
series of stages. Erikson's
Integrity means feeling at
with his life. His wife
theory proposes that life is a
peace with oneself and the
verbalized "Kamao ka
sequence of developmental
world. No regrets or
dong, miskan ana ra na
stages or levels of
recriminations. Despair
akong bana, wala gyud na
achievement. He described
and/or 'Disgust' represent the
siya nagmahay ug taman-
eight stages of development
opposite disposition: feelings
taman sa mga
and in each stage signals a
of wasted opportunities,
nangahitabo sa among
task that must be
regrets, wishing to be able to
kinabuhi. Simple ra nga
accomplished. Our progress
turn back the clock and have
panginabuhi ra ang
through each stage is in part
a second chance. Those who
among panginabuhi pero
determined by our success,
are unsuccessful during this
wala gyud na siya nag
or lack of success, in all the
phase will feel that their life
dahum na mudato.
previous stages. Erikson
has been wasted and will
Kontento na siya sa amo.
also believed that the more
experience many regrets. The Okay na sa iya kay
success an individual has at
individual will be left with
napadako niya ug maayo
each developmental stage,
feelings of bitterness and
among mga anak,
15
the healthier the personality
despair. Those who feel
makahikahos mi sa pang
of an individual is.
proud of their
adlaw-adlaw." Despite of
accomplishments will feel a
it, the patient was not able
sense of integrity.
to send his three children
Successfully completing this
in college. Moreover, the
phase means looking back
patient has been alcoholic
with few regrets and a
for almost 60 years and
general feeling of
been smoking since his
satisfaction. These
teenage years. These
individuals will attain
habits are wasted
wisdom, even when
opportunity and Mr. cutie
confronting death.
has not attained the wisdom since he was not able to decipher that his vices would affect his health in the long run.
16
Robert Havighurst’s Developmental Task Theory Theory
Stage
Result and Justification
Havighurst believes that in
Later Maturity (60 and
The patient has not fully
every developmental stage,
above)
achieved this stage since
certain tasks are needed to be accomplished for one’s progression. In his theory, he proposes that growth and
This stage in a person’s life is concerned with the achievement of the following
each associated with six to ten tasks to be learned. Havighurst identified Six
accomplished. He has his circle of friends whose age is almost same with
tasks:
development is occurring during six stages in life,
some tasks are not
his. They drink and play 1. Adjusting to decreasing physical strength and health. 2. Adjusting to
cards together. But according to his wife, he is not still used to his deteriorating strength. We
Major Stages in human life
retirement and
always wanted to work or
covering birth to old age.
reduced income.
at least to keep his self
Infancy & early childhood (Birth till 6 years old),
3. Adjusting to death of a spouse.
Middle childhood (6-13 years old), Adolescence (13-
busy, same as the thing he has been doing when he was still younger, but his
4. Establishing an
strength is limiting him
18 years old), Early
explicit affiliation
already. Therefore, he was
Adulthood (19-30 years
with one’s age group.
not able to adjust from his
old), Middle Age (3060years old), and Later
5. Meeting civic and social
physical limitation due to aging.
17
maturity (60 years old and over). From there, Havighurst recognized that each human has three
responsibilities. 6. Establishing satisfactory physical living arrangements.
sources for developmental tasks. They are: * Tasks that arise from physical maturation: Learning to walk, talk, control of bowel and urine, behaving in an acceptable manner to opposite sex, adjusting to menopause. * Tasks that arise from personal values: Choosing an occupation, figuring out ones philosophical outlook. * Tasks that have their source in the pressures of society: Learning to read, learning to be responsible citizen. A developmental
18
task is “a task which arises at or about a certain period in the life of an individual, successful achievement of which leads to his happiness and to success with later tasks, while failure leads to unhappiness in the individual, disapproval by society, and difficulty with later tasks”.
JEAN PIAGET’S THEORY OF COGNITIVE DEVELOPMENT Theory
Stage
Result and Justification 19
Jean Piaget proposed a sequence of cognitive development that emphasized the relationship between action and thought. Each phase in his theory is characterized by the ways in which the person interprets and uses the environment. The individual learns by
Formal Operations This stage is characterized by formal reasoning. It is in this stage that a person’s acquisition of the ability to think abstractly, reason logically and draw conclusions from the information available is measured.
The patient did not achieve this cognitive stage. The patient is a chronic alcohol drinker and a smoker. From that alone, he must have thought that this will have a bad effect on his health. He was not able to reason out logically and did not
interacting with the
able to see the bigger
environment through
picture that can be brought
assimilation,
about by his vices that
accommodation and
these will result to illness.
adaptation.
20
DEFINITION OF COMPLETE DIAGNOSIS CAP MR Ascites 2’ Liver Cirrhosis
Community-Acquired Pneumonia Community-acquired pneumonia (CAP) is one of the most common infectious diseases addressed by clinicians. CAP is an important cause of mortality and morbidity worldwide. CAP is usually acquired via inhalation or aspiration of pulmonary pathogenic organisms into a lung segment or lobe. Less commonly, CAP results from secondary bacteremia from a distant source, such as Escherichia coli urinary tract infection and/or bacteremia. CAP due to aspiration of oropharyngeal contents is the only form of CAP involving multiple pathogens. Source: Handbook of Medical-Surgical Nursing 3rd Edition by Springhouse, 2006
Community-Acquired Pneumonia Community-acquired pneumonia (CAP) is a disease in which individuals who have not recently been hospitalized develop an infection of the lungs (pneumonia). CAP is a common illness and can affect people of all ages. CAP often causes problems like difficulty in breathing, fever, chest pains, and a cough. CAP occurs because the areas of
21
the lung which absorb oxygen (alveoli) from the atmosphere become filled with fluid and cannot work effectively. Patients at moderate risk (class IV of the Pneumonia Severity Index) and high risk (class V) should be hospitalized, given their much higher rates of death and complications. In general, most such patients are elderly and have two or more additional poor prognostic factors, such as serious coexisting conditions, abnormal vital signs, and abnormal laboratory values. Source: Medical-Surgical Nursing: A Psychophysiologic Approach by Luckmann and Sorensen, 2003
Community-Acquired Pneumonia Patients with community-acquired pneumonia often present with cough, fever, chills, fatigue, dyspnea, rigors, and pleuritic chest pain. When a patient presents with suspected community-acquired pneumonia, the physician should first assess the need for hospitalization using a mortality prediction tool, such as the Pneumonia Severity Index, combined with clinical judgment. Pneumonia Severity Index
Patient Characteristics
Points
Demographics Male Female
Age (years) Age (years) – 10 22
Patient Characteristics
Points
Nursing home resident Comorbid illness
+ 10
Neoplastic disease Liver disease Congestive heart failure Cerebrovascular disease Renal disease Physical examination findings
+ 30 + 20 + 10 + 10 + 10
Altered mental status Respiratory rate >30 breaths per minute Systolic blood pressure < 90 mm Hg Temperature < 35°C (95°F) or >40°C (104°F) Pulse rate >125 beats per minute Laboratory and radiographic findings
+ 20 + 20 + 20 + 15 + 10
Arterial pH < 7.35 Blood urea nitrogen >64 mg per dL (22.85 mmol per L) Sodium < 130 mEq per L (130 mmol per L) Glucose >250 mg per dL (13.87 mmol per L) Hematocrit < 30 percent Partial pressure of arterial oxygen < 60 mm Hg or oxygen percent
+ 30 + 20 + 20 + 10 + 10 + 10
saturation < 90 percent Pleural effusion Total points:
+ 10 _______ Mortality % (No. of
Recommended site of
Point total
Risk
Risk class patients)
care
No
Low
I
0.1 (3,034)
Outpatient
predictors ≤ 70 71 to 90 91 to 130 >130
Low Low Moderate High
II III IV V
0.6 (5,778) 2.8 (6,790) 8.2 (13,104) 29.2 (9,333)
Outpatient Inpatient (briefly) Inpatient Inpatient
Source: Stephanie Wessel Reyburn, M.D., M.P.H., Mayo School Of Graduate Medical Education, Rochester, Minnesota - Http://Www.Aafp.Org/Afp/2006/0201/P442.Html Accessed On February 21, 2010
23
Ascites Ascites is an accumulation of serous fluid in the abdominal cavity. The fluid accumulates primarily because of low production of albumin by the failing liver. An insufficient amount of protein in the capillaries causes plasma to seep into the abdominal cavity. The accumulated fluid causes a markedly enlarged abdomen. The fluid may cause severe respiratory distress as a result of elevation of the diaphragm. Source: Understanding Medical Surgical Nursing by Williams and Hopper, 2007
Ascites Ascites is the accumulation of fluid (usually serous fluid which is a pale yellow and clear fluid) in the abdominal (peritoneal) cavity. The abdominal cavity is located below the chest cavity, separated from it by the diaphragm. Ascitic fluid can have many sources such as liver disease, cancers, congestive heart failure, or kidney failure. Source: Medical-Surgical Nursing: A Psychophysiologic Approach by Luckmann and Sorensen, 2003
Ascites
24
Ascites is diagnosed by inspection of the fluid-filled abdomen, percussion for dullness and tapping of massive ascites to produce fluid waves. When these signs are accompanied by other manifestations of disease associated with ascites, usually cirrhosis, identification of the problem is validated.
Source: Handbook of Medical-Surgical Nursing 3rd Edition by Springhouse, 2006
Liver Cirrhosis Liver cirrhosis is the final stage of many types of liver injury. The cirrhotic liver varies in appearance, but a nodular consistency with hands of fibrosis (scar tissue) is prominent. The cirrhosis patient frequently presents with problems such as ascites, gastrointestinal bleeding and encephalopathy. The disease often progresses quietly until such as emergency occurs. Hepatomegaly (enlarged liver), splenomegaly (enlarged spleen), vascular changes, or abnormal laboratory tests may be the first indicator in the patient who is
25
Source: Medical-Surgical Nursing: A Psychophysiologic Approach by Luckmann and Sorensen, 2003
Liver Cirrhosis A chronic hepatic disease, cirrhosis is characterized by diffuse destruction and fibrotic regeneration of hepatic cells. As necrotic tissue yields to fibrosis, this disease alters liver structure and normal vasculature, impairs blood and lymph flow, and ultimately causes hepatic insufficiency.
Source: Handbook of Medical-Surgical Nursing 3rd Edition by Springhouse, 2006
Liver Cirrhosis Cirrhosis is a consequence of chronic liver disease characterized by replacement of liver tissue by fibrous scar tissue as well as regenerative nodules (lumps that occur as a result of a process in which damaged tissue is regenerated) leading to progressive loss of liver function.
Source: Blackwell’s Dictionary of Nursing 5th Edition, 2004
26
27
PHYSICAL ASSESSMENT
Date and Time Performed: February 11, 2010 at 5:00 pm Personal Data Cutie is a male patient itted to the Med of Davao Medical Center. He is 72 years old and was born on May 23, 1937. He was born in IGACOS, Davao City and is currently living at Buhangin, Davao City. He is Filipino and a Christian (Roman Catholic) in religion. He is married. The reason for his ission is malaise, loss of appetite, nausea, and black stools experienced on the 6th of February, 2010. Health History The patient claimed that he never had any past illnesses that lead him to an ission to a hospital. It was just a number of feverish experiences, cough, colds and flu which he had. It was stated by his wife upon our interview that he was diagnosed with hypertension a year ago and had maintenance medications. And just a month ago, he then had chest pain, dizziness, nausea, and body malaise. General Survey Received lying on bed unconscious as evidenced by the patient not responding to verbal and pain stimuli. Patient had an IVF of D5NaCl at 80cc/hr infusing well at left metacarpal vein; with endotracheal tube with O2 at 5-7 L/min connected to a bag valve; with Foley catheter connected to a Urobag draining 100 cc of dark yellow colored urine. He was untidy as the patient was with dirty feet and untrimmed and dirty nails. 28
Vital Signs: BP- 110/70mmhg
Temperature- 38.3
PR- 96bpm
RR- 24
Skin The patient had jaundice with uniform skin color all throughout the body except under his axillae, which is darker. His skin folds and axillae were moist. Skin temperature was uniform in all extremities when touched. Senile skin was noted. Hair Upon inspection, hair was short and white in color. His hair was thin and evenly distributed as evidenced by the absence of areas of alopecia along the scalp. No infection or infestations were noted upon inspection and palpation of the patient’s hairline and scalp. Dandruff was noted on patient’s scalp however there were no lesions, lumps, or masses upon palpation. Nails Clubbing of nails was noted on patient. Upon palpation, nail base was firm and fingernails had a rough texture. Epidermis surrounding the nails was intact and no lesions were noted. Nails were long, dirty and untrimmed. Toenail surface was slightly curved and rough.
29
Skull and Face Skull was rounded and normocephalic. Symmetry in anatomy of face was noted. Eyes and Vision Hair of eyebrows was evenly distributed and periorbital skin was intact without swelling or inflammation. Eyebrows were symmetrically aligned. Upon inspection, skin of eyelids was intact and no discharges and discolorations were present. Icteric sclera was noted. Iris were black in color, and had a round, smooth border. Pupillary response to illumination was sluggish and equal on both eyes as evidenced by constricting of both illuminated and non-illuminated pupils upon illumination. Patient does not wear glasses: visual acuity when he was still conscious and awake was grossly normal as stated by his wife. Ears and Hearing Upon inspection, auricles were of the same color with facial skin, were symmetrically aligned with each other, and were aligned with the outer canthus of each eye. Cerumen was present but was not impacted or excessive in amount. Upon palpation, auricles were firm, and not tender as evidenced by the auricle being pulled upward, downward, and backward without resistance, and the pinna being folded forward without resistance and recoiling after folding. Patient was unresponsive since he is in comatose.
30
Nose Upon inspection, external nose was symmetrical. No abnormal discharges or flaring were noted. Also, the nose was with uniform color with facial skin. Nasal septum was intact and in midline. Patient was with NGT on his right nares. Mouth Upon inspection, endotracheal tube with O2 at 5-7 L/min connected to bag valve was noted. Outer lips were brownish pink and were dry. Teeth were shiny and yellow in color. Neck Upon inspection, neck veins were not distended or visible. Shoulder muscles were of anatomically symmetrical. Thorax and Lungs The skin over the posterior thorax was intact and uniform in color with the rest of the body. Also, chest expansion was symmetrical when air is istered through the endotracheal tube with O2 at 5-7 L/min connected to a bag valve. Crackles were noted upon auscultation. Cardiovascular and Peripheral Vascular Peripheral pulses were regular and present on all four extremities. Slow capillary refill time of 4-5 seconds gathered upon three checks was noted.
31
Chest No masses, lesions or any unusuality noted on patient’s chest. Abdomen Upon inspection, distended abdomen and ascites was noted. Abdomen was supple when palpated. Size of abdomen was observed to be not appropriate for patient’s body. Abdominal girth of 39 inches was taken. Caput medusae noted on the skin of the abdomen. Genito-urinary Upon inspection, no swelling, lesion or mass noted on the genitals of the patient. Patient is with Foley catheter which is connected to a Urobag draining 100 cc of dark yellow colored urine. Back and Extremities Patient was not able to manifest movements on the upper body and lower body since the patient was not conscious during the assessment. Bones appear to have no deformities. Elbows have no deformities. However a grade 1 pitting edema was noted on all four extremities as skin does not immediately (approximately 4 seconds) go back to its normal state when pressure is applied.
32
ANATOMY AND PHYSIOLOGY
Liver The liver is the largest internal organ in the body, and weighs about 3 pounds in an adult. The liver is located in the right upper quadrant of the abdomen, just below the diaphragm. A thick capsule of connective tissue called Glisson's capsule covers the entire surface of the liver. The liver is divided into a large right lobe and a smaller left lobe. The falciform ligament divides the two lobes of the liver. Each lobe is further divided into lobules that are approximately 2 mm high and 1 mm in circumference. These hepatic lobules are the functioning units of the liver. Each of the approximately 1 million lobules consists of a hexagonal row of hepatic cells called hepatocytes. The hepatocytes secrete bile into the bile channels and also perform a variety of metabolic functions. Between each row of hepatocytes are small cavities called sinusoids. Each sinusoid is lined with Kupffer cells, phagocytic cells that remove amino acids, nutrients, sugar, old red blood cells, bacteria and debris from the blood that flows through the sinusoids. The main functions of the sinusoids are to destroy old or defective red blood cells, to remove bacteria and foreign particles from the blood, and to detoxify toxins and other harmful substances. Approximately 1500 ml of blood enters the liver each minute, making it one of the most vascular organs in the body. Seventy-five percent 33
of the blood flowing to the liver comes through the portal vein; the remaining 25% is oxygenated blood that is carried by the hepatic artery. The hepatic portal system begins in the capillaries of the digestive organs and ends in the portal vein. Consequently, portal blood contains substances absorbed by the stomach and intestines. Portal blood is ed through the hepatic lobules where nutrients and toxins are absorbed, excreted or converted. Restriction of outflow through the hepatic portal system can lead to portal hypertension. Portal hypertension is most often associated with cirrhosis. Patients usually present with splenomegaly, ascites, GI bleeding and/or portal systemic encephalopathy. The consequences of portal hypertension are due to portal systemic anastomosis formed by the body as an attempt to by the obstructed liver circulation. These collateral vessels form along the falciform ligament, diaphragm, spleen, stomach and peritoneum. The collaterals find their way to the renal vein where blood drained from the digestive organs is let into the systemic circulation. The liver is responsible for important functions, including: •
Bile production and excretion
•
Excretion of bilirubin, cholesterol, hormones, and drugs
•
Metabolism of fats, proteins, and carbohydrates
•
Enzyme activation
34
•
Storage of glycogen, vitamins, and minerals
•
Synthesis of plasma proteins, such as albumin and globulin, and clotting factors
•
Blood detoxification and purification
The liver synthesizes and transports bile pigments and bile salts that are needed for fat digestion. Bile is a combination of water, bile acids, bile pigments, cholesterol, bilirubin, phospholipids, potassium, sodium, and chloride. Primary bile acids are produced from cholesterol. When bile acids are converted or "conjugated" in the liver, they become bile salts. Bilirubin is the main bile pigment that is formed from the breakdown of heme in red blood cells. The broken-down heme travels to the liver, where is it secreted into the bile by the liver. Bilirubin production and excretion follow a specific pathway. When the reticuloendothelial system breaks down old red blood cells, bilirubin is one of the waste products. This "free bilirubin" is a lipid soluble form that must be made water-soluble to be excreted. The conjugation process in the liver converts the bilirubin from a fat-soluble to a water-soluble form. The liver also plays a major role in excreting cholesterol, hormones, and drugs from the body. The liver plays an important role in metabolizing nutrients such as carbohydrates, proteins, and fats. The liver helps metabolize carbohydrates in three ways: •
Through the process of glycogenesis, glucose, fructose, and galactose are converted to glycogen and stored in the liver.
35
•
Through the process of glycogenolysis, the liver breaks down stored glycogen to maintain blood glucose levels when there is a decrease in carbohydrate intake.
•
Through the process of gluconeogenesis, the liver synthesizes glucose from proteins or fats to maintain blood glucose levels.
The liver synthesizes about 50 grams of protein each day, primarily in the form of albumin. Liver cells also chemically convert amino acids to produce ketoacids and ammonia, from which urea is formed and excreted in the urine. Digested fat is converted in the intestine to triglycerides, cholesterol, phospholipids, and lipoproteins. These substances are converted in the liver into glycerol and fatty acids, through a process known as ketogenesis. Prothrombin and fibrinogen, substances needed to help blood coagulate, are both produced by the liver. The liver also produces the anticoagulant heparin and releases vasopressor substances after hemorrhage. Liver cells protect the body from toxic injury by detoxifying potentially harmful substances. By making toxic substances more water soluble, they can be excreted from the body in the urine. The liver also has an important role in vitamin storage. High concentrations of riboflavin or Vitamin B1 are found in the liver. 95% of the body's vitamin A stores are concentrated in the liver. The liver also contains small amounts of Vitamin C, most of the body's Vitamin D stores, and Vitamins E and K.
36
Biliary tract The biliary tract (or biliary tree) is the common anatomy term for the path by which bile is secreted by the liver on its way to the duodenum, or small intestine, of most of the mammal family. It is referred to as a tree because it begins with many small branches which end in the common bile duct, sometimes referred to as the trunk of the biliary tree. The duct is present along with the branches of the hepatic artery and the portal vein forming the central axis of the portal triad. Bile flows in opposite direction to that of the blood present in the other two channels. The liver is usually excluded, but sometimes included. Pressure inside in the biliary tree can give rise to gall stone and lead to cirrhosis of the liver. Blockage can cause jaundice. The biliary tract can also serve as a reservoir for intestinal tract infections. Since biliary tract is an internal organ, it has no somatic nerve supply,and,therefore,colicky pain due to infection and inflammation of the biliary tract is not a somatic pain but it may be caused by luminal distension which causes stretching of the wall (the same mechanism of pain in intestinal colic in intestinal obstruction in which intestine also do not have somatic nerve supply)
37
The path is as follows: •
Bile canaliculi >> Canals of Hering >> bile ductules (in portal tracts) >> intrahepatic bile ducts >> left and right hepatic ducts >>
•
merge to form >> common hepatic duct >>
•
exits liver and s >> cystic duct (from gall bladder) >>
•
forming >> common bile duct >> s with >> pancreatic duct >>
•
forming >> ampulla of Vater >> enters duodenum The anatomy of the biliary tree is a little complicated, but it is important to
understand. The liver's cells (hepatocytes) excrete bile into canaliculi, which are intercellular spaces between the liver cells. These drain into the right and left hepatic ducts, after which bile travels via the common hepatic and cystic ducts to the gallbladder. The gallbladder, which has a capacity of 50 milliliters (about 5 tablespoons), concentrates the bile 10 fold by removing water and stores it until a person eats. At this time, bile is discharged from the gallbladder via the cystic duct into the common bile duct and then into the duodenum (the first part of the small intestine), where it begins to dissolve the fat in ingested food. The liver excretes approximately 500 to 1000 milliliters (50 to 100 tablespoons) of bile each day. Most (95%) of the bile that has entered the intestines is resorbed in the last part of the small intestine (known as the terminal ileum), and returned to the liver for reuse.
38
The many functions of bile are best understood by knowing the composition of bile: 1. Bile Salts (cholates, chenodeoxycholate, deoxycholate): these are produced by the liver's breakdown of cholesterol. They function in bile as detergents that dissolve dietary fat and allow it to be absorbed. Hence, disruption of bile excretion disrupts the normal absorption of fat, a process called malabsorption. Patients develop diarrhea because the fat is not absorbed (steatorrhea) , and develop deficiencies of the fat-soluble vitamins (A, D, E, and K). 2. Cholesterol and phospholipids-while only 4% of bile is cholesterol, the secretion of cholesterol and its metabolites (bile salts) into bile is the body's major route of elimination of cholesterol. Phospholipids, which are components of cell membranes, enhance
the
cholesterol
solubilizing
properties of bile salts. Inefficient excretion of cholesterol can cause an increased serum cholesterol. This predisposes to vascular disease (heart attacks, strokes, etc.) 3. Bilirubin-while this comprises only 0.3% of bile, it is responsible for bile's yellow color. Bilirubin is a product of the body's metabolism of hemoglobin, the carrier of oxygen in red blood cells. Disruption of the excretion of this component of bile leads to a yellow discoloration of the eyes and skin (jaundice). 4. Protein and miscellaneous components
39
Bile production and recirculation is the main excretory function of the liver. Tumors that obstruct the flow of bile from the liver can also impair other liver functions. Therefore, it is necessary to understand these other functions to understand the symptoms that these tumors can cause. These include: Metabolic functions, such as the maintenance of glucose (blood sugar) levels Synthetic functions, such as the synthesis of serum proteins such as albumin, blood clotting (coagulation) factors, and complement (a mediator of inflammatory responses) Storage functions, such as the storage of sugar (glycogen), fat (triglycerides), iron, copper, and fat soluble vitamins (A, D, E, and K) Catabolic functions, such as the detoxification of drugs Circulation of the blood in blood vessels There are two circulatory routes of blood as it flows through the blood vessels: the systemic and the pulmonary circulation. In systemic circulation, blood flows from the left ventricle of the heart through blood vessels to all parts of the body (except gas exchange tissues of lungs) and back to the atrium. In pulmonary circulation on the other hand, venous blood moves from the right atrium to right 40
ventricle to pulmonary artery to lung arterioles and capillaries where gases exchanged; oxygenated blood returns to the left atrium via pulmonary veins; from left atrium, blood enters the left ventricle.
Hepatic Portal Circulation The veins of the hepatic portal digestive
circulation organs,
drain
the
spleen,
and
pancreas and deliver this blood to the liver through the hepatic portal vein. When you have just eaten, the hepatic portal blood contains large amounts of nutrients. Since the liver is a key body organ involve in maintaining the proper glucose, fat and protein concentrations in the blood, this system “takes a detour “to ensure that the liver processes these substances before they enter the systemic circulation. As blood flows slowly through the liver, some of the nutrients are removed to be stored or processed in various ways for later release to the blood. The liver is drained by the hepatic veins that enter the inferior vena cava. Like the portal circulation that links the hypothalamus of the brain and the anterior pituitary gland, the hepatic portal circulation is
41
a unique and unusual circulation. Normally, arteries feed capillary beds, which in turn drain into veins. Here we see veins feeding the liver circulation. The inferior mesenteric vein, draining the terminal part of the large intestine, drains into the splenic vein, which itself drains the spleen, pancreas and the left side of the stomach. The splenic vein and superior mesenteric vein (which drains the small intestine and the first part of the colon) to form the hepatic portal vein. The L. Gastric vein, which drains the right side of the stomach, drains directly into the hepatic portal vein.
42
ETIOLOGY
43
Basic Etiology Predisposing
Present/
Rationale
Actual
Absent
Factors Male
Liver Cirrhosis occurs
The patient is male.
mostly in men. http://www.cancer.org/docr oot/cri/content/cri_2_2_2x_ what_causes_liver_cancer_ 25.asp Ages 45-75
Liver Cirrhosis is most
The patient is 72 years old.
common among people ages Race: Asian
45-75 years old. In Asia and Africa, cirrhosis
The patient is an Asian since
is also common but more
he was born from Filipino
likely to be associated with
parents, and he was born in
hepatitis.
IGACOS, Davao City, and currently resides here in
http://esynopsis.uchc.edu/e
Buhangin, Davao City.
Atlas/GI/1210.htm
Biliary atresia
X
Infants can be born without
The patient has no record or
bile ducts (biliary atresia)
history of Biliary atresia.
and ultimately develop cirrhosis. The bile ducts carry bile formed in the liver to the intestines, where the bile helps in the digestion of fat. So, when the bile ducts are blocked, bile is trapped in the liver, http://www.medicinenet.co m/cirrhosis/page3.htm
44
Basic Etiology Precipitating
Present/
Rationale
Actual
Absent
Factors Chronic
alcoholism
Chronic high levels of alcohol
As stated by the
consumption injure liver cells.
patient’s wife, the
Alcohol seems to injure the liver
patient at his young age
by blocking the normal
was able to drink 1 long
metabolism of protein, fats, and
neck (750 ml) of
carbohydrates. Alcohol can
Tanduay on his own. At
poison all living cells, causing
times, he goes beyond 1
liver cells to become inflamed
long neck and even
and die. Thirty percent of
drinks half a gallon of
individuals who drink daily at
“Tuba” when he is not
least eight to sixteen ounces of
yet drunk. As stated by
hard liquor or the equivalent for
his wife, his husband
fifteen or more years will develop
does not stop drinking
cirrhosis.
unless he becomes drunk. When he reached
http://www.emedicinehealth.com/ cirrhosis/page2_em.htm#Cirrhosi s%20Causes
his adulthood, he continues to drink and smoke when he finds time to do them.
Chronic viral
X
Condition where hepatitis B or
The patient had no
hepatitis
hepatitis C virus infects the liver
medical record of
(types B, C,
for years. some patients infected
acquiring hepatitis B, C,
and D).
with hepatitis B virus and most
or D.
patients infected with hepatitis C virus develop chronic hepatitis, which, in turn, causes progressive
45
liver damage and leads to cirrhosis, and, sometimes, liver cancers. Hepatitis B causes liver inflammation and injury that over several decades can lead to cirrhosis. Hepatitis D is dependant on the presence of hepatitis B, but accelerates cirrhosis in co-infection The hepatitis C virus ranks with alcohol as a major cause of chronic liver disease and cirrhosis. Infection with this virus causes inflammation of and low grade damage to the liver that over several decades can lead to cirrhosis. http://www.spiritustemporis.com/cirrhosis/causes.ht ml
46
Smoking
Research reveals that smoking
The patient smokes 1-2
damages the liver. Smoking
packs of cigarette a day,
activates chemical materials
and he started smoking
within the body. These chemicals
when he was a teenager.
that are manufactured by smoking At the same time, he also provoke oxidative stress
also drinks Tanduay
which is linked with lipid
(750mL) 2-3 times a
peroxidation. When this occurs,
week since he was a
the condition fibrosis is
teenager. He only
developed.
stopped smoking when
Smoking increases the manufacturing of pro-
he was diagnosed with hypertension last 2009.
inflammatory cytokines which is related to liver cell damage. Smoking also contributes the continued succession of chronic alcoholic-hepatitis as well as to the progression of cirrhosis.
Http://www.ehow.com/howdoes_4577854_effects-smokingdrinking-liver.html
47
Malnutrition, especially
X
Fat builds up in the liver and
There is no scientific
eventually causes cirrhosis.
basis that the patient has
high fat intake
an increase fat in the Fat (triglycerides) accumulates throughout the hepatocytes for the following reasons: •
Export of fat from the
blood or increased level of cholesterol in the blood (LDL-bad cholesterol)
liver is decreased because hepatic fatty acid oxidation and lipoprotein production decrease. •
Input of fat is increased because the decrease in hepatic fat export increases peripheral lipolysis and triglyceride synthesis, resulting in hyperlipidemia.
http://digestive.niddk.nih.gov/ddi seases/pubs/cirrhosis/
48
SYMPTOMATOLOGY
SYMPTOMS
Present/
Rationale
Actual
absent Anorexia
Increased brain tryptophan (TRP)
This is present
availability for serotonin synthesis
with the patient,
play a role in the pathogenesis of
since this is one
anorexia. Since in chronic liver
of the reasons he
failure, increased plasma and
consulted the
cerebrospinal fluid TRP
emergency room.
concentrations are characteristically
The wife stated
reported, that also in liver cirrhosis,
that the patient
increased brain TRP availability
had no appetite to
constitute the pathogenic mechanism
eat
of anorexia.
http://www3.interscience.wiley.com/j ournal/49716/abstract? CRETRV=1&SRETRY=0 Nausea and vomiting
The malabsorption of fats may lead
Two weeks prior
to deficit of fatsoluble vitamins,
to ission, the
hemorrhoids, intolerance to fatty
patient started
foods, nausea and vomiting attacks,
feeling nauseous,
and abdominal bloating. Since the
and four days
liver has already decreased in
prior to
function, its function to produce bile
ission, he had
which emulsifies fats is also
prandial vomiting
decreased, thus these symptoms
which is one of
persists.
the reasons he
49
www.enwikipedia.org/wiki/Liver_dis
sought
ease#Symptoms_of_a_diseased_liver
consultation at the emergency room.
Body malaise
This is due to the decreased in liver
The patient
function of the liver because of the
experienced body
hepatic fibrosis. Therefore, the
malaise, and was
patient has also decreased
one of his chief
erythropoietin which then results to
complaint that
the decrease of red blood cells
resulted to his
circulating in the blood, and there
ission at
will be decreased hemoglobin. All of
DMC.
this in return will cause the patient to have body malaise. Bleeding
tendencies
Bleeding tendencies such as
The patient had
nosebleeds, easy bruising, and
bleeding as
bleeding gums may result from
evidenced by him
thrombocytopenia secondary to
having black
splenomegaly, decreased vitamin K
stools, which is
absorption and decreased production
also known as
of coagulation factors and
melena, indicative
regurgitation of blood to the spleen
of bleeding in the
and gastrointestinal tract.
upper gastrointestinal tract.
Suddarth, Doris Smith. The Lippincott Manual of Nursing Practice. 5th edition. 1991. Pages 514515.
Portal
Portal hypertension occurs because of The patient has
50
hypertension
the obstruction of portal circulation
ascites which is a
brought about by the portal
complication of
obstruction caused by the hepatic
portal
scarring.
hypertension.
http://www.emedicinehealth.com/cirr hosis/page2_em.htm#Cirrhosis %20Causes
This is an evidence that he indeed has portal hypertension. In addition, the patient was diagnosed to have hypertension on the year 2009.
Ascites
This
happened
because
of
the The patient has
decrease of albumin in the blood ascites as plasma. Albumin is responsible for evidenced by his maintaining the oncotic pressure in distended the blood volume. A decrease in abdominal cavity. albumin will mean a decrease in oncotic pressure, which will result to a more permeable membrane which results to fluid leaking through the vasculature
into
the
abdominal
cavity. Suddarth, Doris Smith. The Lippincott Manual of Nursing Practice. 5th edition. 1991. Pages 514515. Jaundice
Jaundice is the buildup of bile
The patient was
pigment that is ed by the liver
noted to have 51
into the intestine. Due to the portal
yellowish skin
obstruction, the bile going to the GI
color on all four
tract will have a backflow to the
extremities
liver. The bile then goes to the blood
including the
stream, and this causes the yellowing
palms. The
of the skin, due to the presence of bi
patient also had icteric sclera
(http://www.healthscout.com/ency/68
when inspected.
/292/main.html)
edema on the
extremities
Plasma albumin is reduced, leading One week prior to to edema.
ission, the wife of the patient
Suddarth, Doris Smith. The
noticed the
Lippincott Manual of Nursing
obvious
Practice. 5th edition. 1991. Pages 514- abdominal 515.
distention of the patient’s abdomen. Upon physical assessment, the patient was noted to have ascites and edema on all four extremities.
Caput medusae
Portal hypertension results from the
The patient was
abnormal blood flow pattern in liver
noted to have
created by cirrhosis. The increased
large, dilated, and
pressure is transmitted to collateral
distended veins
venous channels. Sometimes these
on the abdomen
venous collaterals are dilated. Caput
area when
52
medusa consists of dilated veins seen
inspected
on the abdomen of a patient with cirrhosis of the liver.
Coma
This is a progressive symptom, The patient is on a secondary to the loss of ammonia to comatose state. urea
conversion
and
consequent
delivery of toxic ammonia to the brain. Deterioration of mental function from lethargy to coma and eventual death
PATHOPHYSIOLOGY
53
PATHOPHYSIOLOGY
54
DOCTOR’S ORDERS DATE
DOCTOR'S
RATIONALE
REMARKS
ORDER Feb. 6,
Please it patient ission in the hospital is required
2010
under blue service – for optimum medical and nursing care;
ITTED
55
Level II Pavillion and to receive medications, undergo tests, and perform procedures which can only be done in the hospital setting. The blue service accommodates patients with gastro, endo and immunologic problems. VSq4 and record
Vital signs are taken to provide
TAKEN
please
baseline data and to watch-out for any
AND
unusualities.
RECORDED
Start venoclysis with Helps expand intravascular volume, PNSS 1L @
corrects an underlying imbalance in
120cc/hr
fluids and electrolytes and compensates
STARTED
the loss in the body. Moreover, it serves as a route for medication. Labs:
CBC (complete blood count and
CBC PC
platelet count) is a basic screening test WITH and is one of the most frequently
DONE
RESULTS
ordered laboratory procedures. The findings in the CBC PC give valuable diagnostic information about the hematologic and other body systems, prognosis, response to treatment and recovery. CXR-PA
A chest radiograph is used to diagnose DONE BUT
56
conditions affecting the chest, its
NO
contents, and nearby structures. Chest
IMPRESSIO
radiographs are among the most
N MADE
common films taken, being diagnostic of many conditions. A chest x-ray may be ordered when a person's symptoms include a persistent cough, coughing up blood, chest pain, a chest injury, or difficulty in breathing. ECG
ECG is a non-invasive test used to
NOT DONE
assess the heart function. It is a graphic produced by an electrocardiograph, which records the electrical activity of the heart over time. B1 B2
Elevation of serum bilirubin levels is
DONE
related to hemolysis of RBCs and
WITH
subsequent re-absorption of
RESULTS
unconjugated bilirubin from the small intestines. The condition may be benign or may place the patient at risk for multiple complications/untoward effects.
57
BUN
The BUN test is primarily used, along DONE with the creatinine test, to evaluate
WITH
kidney function in a wide range of
RESULTS
circumstances, to help diagnose kidney disease, and to monitor patients with acute or chronic kidney dysfunction or failure. Increased BUN levels suggest impaired kidney function. This may be due to acute or chronic kidney, damage, or failure. S. Na, S. K
Serum sodium and serum potassium
NOT DONE
levels are checked to determine fluid and electrolyte balance. Crea
A disorder in the kidney function
NOT DONE
reduces excretion of creatinine, resulting in increased blood creatinine levels. This test diagnoses impaired renal functions. SGPT and SGOT
Elevations of SGPT, an enzyme found DONE within the liver cells, indicate that the WITH liver cells are either leaky (internal
RESULTS
contents are entering the blood) or damaged.
58
Meds:
Inhibits reabsorption of sodium and
Furosemide 40 mg
chloride at proximal and distal tubule
tab OD
and in the loop of Henle
Spironolactone
Spironolactone inhibits the action of
25mg tab OD
aldosterone thereby causing the kidneys
GIVEN
GIVEN
to excrete salt and fluid in the urine while retaining potassium. Essentiale Forte
Increase functional status of the liver,
CAP BID
improvement in the lipids metabolism
GIVEN
caused by accelerated synthesis of lipoproteins in the liver, activation of the phospholipid-depending ferments, increased synthesis of glycogen in the liver, decreased the fatty infiltration of the hepatocytes I&O q shift
Intake & output monitoring is done to
RECORDED
assess the fluid retention status of the patient and to prevent cardiac overload. Watch out for any
To ensure that immediate nursing
WATCHED
unsualities
interventions can be rendered in cases
OUT
of deviances from the normal health status so complications can be prevented Refer accordingly
Referral is done to correct unusualities
REFERRED
as soon as possible and to inform the
59
attending physician of the patient's condition. February Labs: CBC PC,
These tests were not yet done and so
7, 2010
ECG, B1 B2, S. Na, the doctor ordered again and made
@ 4:00
K, Crea, SGPT,
AM
SGOT
NOT DONE
requests for these tests for analysis.
Follow up chest X-
This is to inform the patient or
FOLLOWED
ray reading
significant other to have the copy of the UP result from the laboratory.
Additional labs: 1.
Transabdominal USD is ordered to for NOT DONE
Transabdominal
visualization of the abdomen which
USD
helps in diagnosing the patient’s condition.
2. Serum albumin
A serum albumin test measures the
DONE
amount of this protein in the clear
WITH
liquid portion of the blood. This test
RESULTS
can help determine if a patient has liver disease or kidney disease, or if the body is not absorbing enough protein. 3. HBS-Ag
The hepatitis B surface antibody (anti- NOT DONE HBs) is the most common test. Its presence indicates previous exposure to HBV, but the virus is no longer present and the person cannot on
60
the virus to others. 4. Anti-HAV IgM
This test is used to help diagnose a
NOT DONE
liver infection due to the hepatitis A virus (HAV). This test may also be used to determine if you have produced antibodies and developed immunity in response to a hepatitis A vaccine or a previous hepatitis A infection. 6. Anti-HCV
To determine if you have contracted
NOT DONE
the hepatitis C virus (HCV) and to monitor treatment of the infection 7. PT/PTT
Since the Prothrombin time (PT)
NOT DONE
evaluates the ability of blood to clot properly, it can be used to help diagnose bleeding. When used in this instance, it is often used in conjunction with the PTT to evaluate the function of all coagulation factors. Occasionally, the test may be used to screen patients for any previously undetected bleeding problems prior to surgical procedures.
61
Furosemide 40mg
Inhibits reabsorption of sodium and
IVTT now, then
chloride at proximal and distal tubule
GIVEN
Furosemide 40mg 1 and in the loop of Henle tab BID Spironolactone
Spironolactone inhibits the action of
100mg BID
aldosterone thereby causing the kidneys
GIVEN
to excrete salt and fluid in the urine while retaining potassium. Essentiale Forte 1
Increase functional status of the liver,
cap TID
improvement in the lipids metabolism
GIVEN
caused by accelerated synthesis of lipoproteins in the liver, activation of the phospholipid-depending ferments, increased synthesis of glycogen in the liver, decreased the fatty infiltration of the hepatocyte Lactulose 30cc @
Produces osmotic effect in colon.
bedtime
Resulting distention promotes
GIVEN
peristalsis. Decrease blood ammonia build- up causes hepatic encephalopathy, probably ass result of bacterial degradation which lowers pH of colon contents. Ceftriaxone 1gm
This antimicrobial agent inhibits
GIVEN
62
IVTTq12, ANST
bacterial cell wall synthesis by binding to one or more of the penicillinbinding proteins (PBPs) which in turn inhibits the final transpeptidation step of peptidoglycan synthesis in bacterial cell walls, thus inhibiting cell wall biosynthesis. Bacteria eventually lyse due to ongoing activity of cell wall autolytic enzymes (autolysins and murein hydrolases) while cell wall assembly is arrested.
Please monitor I&0
Intake & output monitoring is done to
MONITORE
q shift and record
assess the fluid retention status of the
D
patient and to prevent cardiac overload. Refer if UO < 30
A decrease in urine output may indicate REFERRED
cc/hr
a serious, even life-threatening condition. It may be caused by dehydration du, diarrhea, lack of adequate fluid intake or total urinary tract obstruction.
CBG q6 (6AM-
The capillary blood glucose test is
11AM- 6PM –
ordered to measure the amount of
11PM)
glucose in the blood right at the time
NOT DONE
of sample collection. It is used to
63
detect both hyperglycemia and hypoglycemia , to help diagnose diabetes, and to monitor glucose levels. Refer if CBG ≥
High levels of glucose most frequently REFERRED
180mg/dL, <
indicate diabetes, but many other
80mg/dL
diseases and conditions can also cause elevated glucose such as chronic renal failure and hyperthyroidism. Low blood glucose levels are seen in patients with drinking alcohol and extensive liver disease.
Refer
Referral is done to correct unusualities
REFERRED
as soon as possible and to inform the attending physician of the patient's condition. February Please do gastric
Gastric lavage is done to address
7, 2010
lavage now until
gastrointestinal bleeding.
@ 8:10
water is clear
AM
DONE
Please insert FBC
To monitor the intake and output of the INSERTED
F16 and attach to
patient. This may also avoid bladder
urobag
distention.
64
Strict I&O
Intake & output monitoring is done to
MONITORE
monitoring and
assess the fluid retention status of the
D AND
record please
patient and to prevent cardiac overload. RECORDED
NPO Temporarily
For better visualization of the abdomen DONE during the ultrasound
Shift IVF to D5NSS D5NSS restores sodium chloride deficit SHIFTED 1L @ 80cc/hr
and extra cellular fluid volume.
For USD of the
Abdominal ultrasound is an imaging
whole abdomen,
procedure used to examine the
KUB, Pancreas
presence of abnormalities in the
NOT DONE
structure of the organs intraabdominally. Continue other meds All medications previously ordered by attending physician should be
CONTINUE D
continued to hasten patient's recovery. Please attach all labs For monitoring and analysis of the requested
ATTACHED
patient’s condition through the results of the tests done
Feb. 8,
Start omeprazole
Suppress gastric acid secretion by
2010 @
40mg IVTTq12, 1st
inhibiting the partial cell H+/K+ ATP
6:20 AM done once available
STARTED
pump
*coffeeground output / NGT 65
Feb. 9,
Repeat CBC,
These tests were not yet done and so
2010 @
protime, USD of the the doctor ordered again and made
11:00
liver, Pancreas,
AM
serum albumin,
NOT DONE
requests for these tests for analysis.
BUN Lactulose 30cc TID, Produces osmotic effect in colon. to make 4-5 bowl
Resulting distention promotes
mvt/day
peristalsis. Decrease blood ammonia
GIVEN
build- up the causes hepatic encephalopathy, probably ass result of bacterial degradation which lowers pH of colon contents. Furosemide 40 mg
Inhibits reabsorption of sodium and
IVTT, OD
chloride at proximal and distal tubule
GIVEN
and in the loop of Henle Omeprazole 40mg
Suppress gastric acid secretion by
IVTT q12
inhibiting the partial cell H+/K+ ATP
GIVEN
pump Vit. K 1 amp IVTT
It is given to prevent bleeding.
GIVEN
OD Essential Forte 1 cap Increase functional status of the liver, TID
GIVEN
improvement in the lipids metabolism caused by accelerated synthesis of lipoproteins in the liver, activation of the phospholipid-depending ferments,
66
increased synthesis of glycogen in the liver, decreased the fatty infiltration of the hepatocytes Metronidazole
Disrupts DNA and protein synthesis
500mg 1 TAB q6
susceptible organisms. Therapeutic
GIVEN
effects: Bactericidal, trichomonacidal or amebicidal action. Spectrum: Most notable for avtivity against anaerobic bacteria including: Bacteroides, clostridium. In addition is active against: Trichomonas vaginalis, entamoeba histolytica, giardia lamdia, H. pylori and clostridium difficile. Hold all PO Meds
Holding all PO meds is done as
DONE
preparation for the gastric lavage. Giving medications would just be drawn out of the patient’s stomach during the procedure. Pls. do gastric lavage Gastric lavage is done to address
DONE
until gastric aspirate gastrointestinal bleeding. goes out clear NPO temporarily
For better visualization of the abdomen DONE during the ultrasound
CBG Monitoring q6 The capillary blood glucose test is ordered to measure the amount of
NOT MONITORE
67
glucose in the blood right at the time
D
of sample collection. It is used to detect both hyperglycemia and hypoglycemia , to help diagnose diabetes, and to monitor glucose levels. Refer for persistent ↓ To notify the physician regarding the in sensorium
REFERRED
changes of the patient’s health status and to prevent further complications
Feb. 9,
Restrain if necessary Patient may be restless or
2010 @ (per watcher’s
uncomfortable with the equipment
12:05
attached to him needing a restraint to
request)
PM
RESTRAINE D
keep them in place and prevent dislodging causing harm.
Feb. 10, Repeat CBC Plt Ct,
These tests were not yet done and so
2010 @
Protime with INR,
the doctor ordered again and made
1PM
Serum Na, K, Crea,
requests for these tests for analysis.
ABG
Blood gases are a measurement of
NOT DONE
DONE
how much oxygen and carbon dioxide is in your blood. It also determines the acidity (pH) of your blood. The test is used to evaluate respiratory diseases and conditions that affect the lungs. It helps determine the effectiveness of
68
oxygen therapy. The test also provides information about the body's acid/base balance, which can reveal important clues about lung and kidney function and the body's general metabolic state. Please facilitate
To conduct ultrasound testing to the
FACILITAT
transport on USD
patient which may be helpful in
ED
test today
determining other problems in the patient’s health status
NPO temporarily
For better visualization of the abdomen DONE during the ultrasound
Give tranexamic
Inhibits activation of plasminogen,
GIVEN
acid 100mg IVTT q8 thereby preventing the conversion of plasminogen to plasmin Give Vit. K 1 amp
It is given to prevent bleeding.
GIVEN
now, OD For gastric lavage
This is to ensure that the patient would DONE
today without fail
undergo the gastric lavage as it is needed by the patient immediately on the same day as per doctor’s request
NPO except meds
Restrictions for any intake per orem
DONE
except the medications is given for better visualization of the abdomen during the ultrasound and for patient’s
69
recovery through the therapeutic effects of medicine. Start albumin 25%
To compensate for the decreased
50 cc q12
albumin levels which is responsible for
STARTED
maintaining osmotic pressure inside the blood vessels BP monitoring qh
To monitor changes in the blood
MONITORE
until stable
pressure which is significant in
D
determining the patient’s status Continue meds
All medications previously ordered by
CONTINUE
attending physician should be
D
continued to hasten patient's recovery. Refer
Referral is done to correct unusualities
REFERRED
as soon as possible and to inform the attending physician of the patient's condition. Feb, 10, Referred for ↓
Glasgow Coma Scale or GCS, is
2010
sensorium, (E1 V3
neurological scale which aims to give
M5) GCS 9
a reliable, objective way of recording
CR – 90
the conscious state of a person, for
RR – 22
initial as well as subsequent
T- 39
assessment. (E1 – does not open eyes,
REFERRED
V3- Utters inappropriate words, M5 Localizes painful stimuli) Moderate Brain Injury, GCS 9 – 12
70
Do ABG now
Blood gases are a measurement of
DONE
how much oxygen and carbon dioxide is in your blood. It also determines the acidity (pH) of your blood. The test is used to evaluate respiratory diseases and conditions that affect the lungs. It helps determine the effectiveness of oxygen therapy. The test also provides information about the body's acid/base balance, which can reveal important clues about lung and kidney function and the body's general metabolic state. Do CBG now
The capillary blood glucose test is
NOT DONE
ordered to measure the amount of glucose in the blood right at the time of sample collection. It is used to detect both hyperglycemia and hypoglycemia , to help diagnose diabetes, and to monitor glucose levels. O2 inhalation @ 5-7 O2 inhalation is indicated for patients
DONE
L/min via face mask that lack oxygen supply and need assistance in maintain the desired
71
oxygen supply Monitor VS qh and
The patient is for close monitoring and MONITORE
record
needs further assessment to monitor to D address if there’s any unusualities
Refer
Referral is done to correct unusualities
REFERRED
as soon as possible and to inform the attending physician of the patient's condition. Feb. 11, Follow-up requested For monitoring and analysis of the
FOLLOWED
2010
-UP
labs
patient’s condition through the results of the tests done
For gastric lavage
Gastric lavage is done to address
DONE
gastrointestinal bleeding. Cold water is used to prevent any bleeding in the gastrointestinal tract. IVF of PNSS 1L @
Helps expand intravascular volume,
80cc/hr
corrects an underlying imbalance in
DONE
fluids and electrolytes and compensates the loss in the body. Moreover, it serves as a route for medication
PNSS is isotonic with the blood and tissue fluid, used as a solvent for drugs that are to be istered parenterally
72
like blood to replace body fluids. It is used as a prime once on blood transfusion. Refer
Referral is done to correct unusualities
REFERRED
as soon as possible and to inform the attending physician of the patient's condition. Feb. 11, Referred due to dec. Glasgow Coma Scale or GCS, is 2010
sensorium GCS5 (E1 neurological scale which aims to give
(+)
V1 M3) & dyspnea
REFERRED
a reliable, objective way of recording
active
the conscious state of a person, for
bleeding
initial as well as subsequent
per orem
assessment. E1- Does not open eyes, V1 - Makes no sounds, M3 -
(+) gross
Abnormal flexion to painful stimuli
hematuri
(decorticate response), GCS of 5 –
a on FC
Severe Brain Injury Intubate pt. now
The ET tube is inserted into a
with ET size 75 level patient's trachea in order to ensure that 21
INTUBATE D
the airway is not closed off and that air is able to reach the lungs. The endotracheal tube is regarded as the most reliable available method for protecting a patient's airway.It is
73
indicated when the oxygenation with noninvasive methods is inadequate CAB while awaiting This is to provide the patient with
DONE
mech. vent. adequate oxygen supply through continues bag valving until the mechanical ventilation is available. MV Set-up
To assist the patient in his breathing
PO2 = 100%
pattern since he is not able to
RR 16
his own required oxygen levels.
DONE
TV 500cc Insert NGT French
Nasogastric intubation is a medical
INSERTED
16 and open to drain process involving the insertion of a plastic tube (nasogastric tube, NG tube) through the nose, past the throat, and down into the stomach. The main use of a nasogastric tube is for feeding and for istering drugs and other oral agents. NPO Temp
For better visualization of the abdomen DONE during the ultrasound
Give tranexamic
Inhibits activation of plasminogen,
acid 500mg IVTT
thereby preventing the conversion of
GIVEN
plasminogen to plasmin
74
Vit. K 1amp IVTT
It is given to prevent bleeding.
GIVEN
Suction catheter –
To remove retained secretion in the
SUCTIONE
PRN
catheter to clear obstructed airway
D
Turn to sides q2
Turning the patient to sides prevents
DONE
now – hold
the patient from developing decubitus ulcer. Continue meds
All medications previously ordered by
CONTINUE
attending physician should be
D
continued to hasten patient's recovery. Refer
Referral is done to correct unusualities
REFERRED
as soon as possible and to inform the attending physician of the patient's condition. Feb. 11, Transfer to 6 or 9 To provide better care and monitoring
TRANSFER
2010 @
awaiting for ICU
to the patient while awaiting for room
RED
12NN
vacancy
vacancy in the ICU
For referral to
For co-management and thorough
consultant c/o Dr.
analysis of the patient’s condition.
INFORMED
Honcoda today To receive 2U PRBC In order to increase the number of red
TRANSFUS
and transfuse once
blood cells in the blood
ED
To secure 6U FFP
For the treatment of deficiencies of
SECURED
and transfuse once
coagulation proteins for which specific
available
factor concentrates are unavailable or
available
75
undesirable. Give tranexamic
Inhibits activation of plasminogen,
acid 500mg IVTT
thereby preventing the conversion of
q8, 1 dose now
plasminogen to plasmin
For gastric lavage
Gastric lavage is done to address
with cold water
gastrointestinal bleeding. Cold water
GIVEN
DONE
is used to prevent any bleeding in the gastrointestinal tract. Referral to Dr.
For co-management and thorough
Pilapil
analysis of the patient’s condition.
For HBS-AG, Anti-
These tests were not yet done and so
HBC IgM, Anti-
the doctor ordered again and made
HCV
requests for these tests for analysis.
For USD of the
Abdominal ultrasound is an imaging
whole ABD
procedure used to examine the
REFERRED
NOT DONE
NOT DONE
presence of abnormalities in the structure of the organs intraabdominally. Pls. facilitate transfer To provide better care to the patient in
FACILITAT
to IMCU/ICU
ED
a setting where he will monitored thoroughly.
Feb. 11, Paracetamol 300mg
Inhibits the synthesis of prostaglandins GIVEN
2010 @
that may serve as mediators of pain and
12:45P
IVTT now
fever, primarily in the CNS.
76
M
Refer
Referral is done to correct unusualities
REFFERED
as soon as possible and to inform the T – 38.2
attending physician of the patient's condition.
Feb. 12, Dx: HBS-Ag, Anti-
These tests were not yet done and so
2010 @
the doctor ordered again and made
HBC, Anti-HCV
11:45 AM
DONE
requests for these tests for analysis. Still for mech. vent.
To provide the patient with adequate
amount of oxygen
Follow up
For compatibility testing.
FOLLOWED
crossmatching of
Crossmatching is important to detect
-UP
blood and transfuse
agglutination of donor RBC’s caused
once available
by antibodies in patient's serum.
For compliance to
Continuation of medication ensure INFORMED
medication
spontaneous condition
treatment
and
of
compliance
DONE
patients to
the
medical regimen, revealing the desired outcomes Refer
Referral is done to correct unusualities
REFERRED
as soon as possible and to inform the attending physician of the patient's condition.
77
DIAGNOSTIC EXAMS Arterial Blood Gas Arterial Blood Gas Test is done to determine an imbalance in the amount of oxygen gas (O2) or carbon dioxide gas (CO2) in your blood or an acid-base imbalance, which may indicate a respiratory (lung/breathing), metabolic, or kidney disorder. Blood gas tests are ordered when there are symptoms of an O2/CO2 or pH imbalance, such as difficulty breathing or shortness of breath. Date ordered: February10, 2010
pH
Value
Normal Range
Unit
7.510
7.35-7.45
mmHg
Clinical Significance
Increase in pH is brought about by the increase in bilirubin in the blood which is alkalinic.
pC02
21.3
35-45
mmHg
Decreased pC02 is caused by hypoxia due to the accumulated fluid in the abdominal cavity creating pressure in the diaphragm. Thus, affecting the respiratory status of the patient.
PO2
82.0
80-100
mmHg
PO2 level is at normal range.
78
HC03
16.6
22.0-27.0
mmol/L
When bicarbonate levels are lower than normal, it suggests that the body is having trouble maintaining its acid-base balance. Bicarbonate concentrations in the serum may fall due to consumption by combining with protons (H+) from acids such as lactic acid, keto-acids etc; or by loss from the body from gastro-intestinal or renal sources. Renal loss of bicarbonate may be due to compensatory mechanisms for a respiratory alkalosis.
02Sat
97.2%
80-100
%
02 Saturation is at normal range.
Partially Compensated Respiratory alkalosis Respiratory alkalosis is a medical condition in which increased respiration (hyperventilation) elevates the blood pH (a condition generally called alkalosis). Respiratory alkalosis is due to the dyspnea caused by the pressure exerted by the ascites to the diaphragm, leading to respiratory rate which is lower than normal. Moreover, respiratory alkalosis could result from a ventilatory rate or tidal volume that is too high or from the patient triggering excessive additional breaths.
79
Nursing Responsibilities when withdrawing blood o
order and patient identity
o Explain to the patient the purpose of the hematology or blood test. o
Gather equipment and wear clean gloves
o Inform the patient that the blood sample will be drawn from his antecubital vein in either of the arms. o Apply hot or cold compress to injection site if swelling occurs. o Inform the patient that a total of 5cc of blood will be extracted from him. o Label the sample and maintain chain of custody and deliver or send sample to the lab o Properly dispose of used equipment
80
Hematology
Hematology is the study of blood and its disorders. Hematologists, board-certified internists, look specifically at blood components such as blood count, and blood and bone marrow cells. Hematology tests can help diagnose anemia, hemophilia, blood-clotting disorders, and leukemia. Date ordered: February 6, 2010
81
TEST
RATIONALE
REFERENCE RESULT
N/H/L CLINICAL SIGNIFICANCE
RANGE CBC+PLT Hgb
Hemoglobin is the protein molecule
115-175 g/L
104
L
Low hemoglobin is referred to
in red blood cells that carries oxygen
as anemia which may by the
from the lungs to the body's tissues
decreased erythropoietin caused by
and returns carbon dioxide from the
cirrhosis of the liver.
tissues to the lungs. Hemoglobin also plays an important role in maintaining Hct
RBC count
the shape of the red blood cells. Hematocrit is a measure of how much
0.36-0.52
0.29
L
Because of the decrease in the RBC
space red blood cells take up in the
in the blood, hematocrit as well
blood.
would decrease.
RBC count is the number of red blood 4.20-6.10 cells per volume of blood, and is
2.94
L
x106 /uL
A decreased number of RBCs results from the decrease erythropoietin
reported in either millions in a
production of the liver.
microliter or millions in a liter of blood. WBC count
Measures the amount of white blood
5.0-10.0 x103
cells. These immune cells form in
/uL
9.65
N
WBC is in normal range.
the bone marrow to help fight infection DIFFERENTIAL COUNT
82
83
TEST
RATIONALE
REFERENCE RESULT
N/H/L CLINICAL SIGNIFICANCE
RANGE CBC+PLT Hgb
Hemoglobin is the protein molecule
115-175 g/L
107.0
L
Low hemoglobin is referred to
in red blood cells that carries oxygen
as anemia which may by the
from the lungs to the body's tissues
decreased erythropoietin caused by
and returns carbon dioxide from the
cirrhosis of the liver.
tissues to the lungs. Hemoglobin also plays an important role in maintaining Hct
RBC count
the shape of the red blood cells. Hematocrit is a measure of how much
0.36-0.52
0.31
L
Because of the decrease in the RBC
space red blood cells take up in the
in the blood, hematocrit as well
blood.
would decrease.
RBC count is the number of red blood 4.20-6.10 cells per volume of blood, and is
3.08
L
x106 /uL
A decreased number of RBCs results from the decrease erythropoietin
reported in either millions in a
production of the liver.
microliter or millions in a liter of blood. WBC count
Measures the amount of white blood
5.0-10.0 x103
cells. These immune cells form in
/uL
12.78
H
High levels indicate presence of bacterial infection.
the bone marrow to help fight infection DIFFERENTIAL COUNT
84
Date ordered: February 9, 2010
85
Blood Chemistry Blood chemistry is the chemical composition of the blood. The levels of various substances in the blood can provide clues to a patient's condition, ranging from the presence of a liver disorder to a pregnancy. Routine bloodwork to check blood chemistry is often a part of a diagnostic workup, with the blood being analyzed to check for specific elements which could contribute clues to the diagnosis. Doctors rely on information about normal ranges of things like proteins and lipids to read the blood analysis. Date ordered: February 9, 2010 TEST
RESULT
UNIT
NORMAL
L/N/H
CLINICAL SIGNIFICANCE
L
Low total protein levels can
RANGE TOTAL PROTEIN
59.40
g/L
63 - 82
suggest a liver disorder. In Total protein measurements can reflect
patients with liver problems,
nutritional status and may be used to
there is a decrease in total
screen for and help diagnose kidney
protein levels because of the
disease, liver disease, and many other
decrease in production of
conditions
albumin, a protein which is
86
exclusively produced in the liver. GLOBULIN
40.70
g/L
23 - 35
H
An elevation in the level of serum globulin can indicate the
Globulins are proteins that include
presence of cirrhosis of the liver
gamma globulins (antibodies) and a
and bacterial infection.
variety of enzymes and carrier/transport proteins. They are a diverse group of proteins in the blood, and together represent the second most common proteins in the bloodstream. ALBUMIN
18.70
g/L
35 - 50
L
There is a decrease of albumin in the blood plasma because of
Albumin is the most abundant protein
the decrease in its production
found in blood plasma, representing 40
due to problems in the liver.
to 60% of the total protein. A/G RATIO
0.5
-
1.5 – 2.5
L
A decrease in Albumin
87
Globulin Ratio is an indicative The ratio of the concentrations of
of a problem in liver functions.
albumin to globulin in blood serum.
88
Blood Chemistry Date ordered: February 6, 2010
89
SGPT
Result
Unit
Reference Ranges
L/N/H
Clinical Significance
84.0
U/L
30.0-65.0
H
An increase in SGPT level is due to impaired liver function caused by liver cirrhosis. It can be
ALT (SGPT) is, by caused by hepatic inflammation (including contrast, normally found infectious mononucleosis, pancreatitis, alcohol, largely in the liver. This viral hepatitis) is not to say that it is exclusively located in liver but that is where it is most concentrated. It is released into the bloodstream as the result of liver injury. It therefore serves as a fairly specific indicator of liver status. SGOT
182.0
U/L
15.0-37.0
H
An increase in SGPT level is due to impaired liver function caused by liver cirrhosis. It can be
AST (SGOT) is normally
caused by hepatic inflammation (including
found in a diversity of
infectious mononucleosis, pancreatitis, alcohol,
tissues including liver,
viral hepatitis)
heart, muscle, kidney, and brain. It is released
90
91
DRUG STUDY
Deneric Name
Brand Name Classification
Furosemide Furoside, Lasix Myrosemide, Uritol, Diumide-K® (functional) Loop diuretic
(chemical) Sulfonamide derivative Dosage and Route 40 mg tab OD Mechanism of Inhibits reabsorption of sodium and chloride at proximal and distal tubule Action and in the loop of Henle Indication Pulmonary edema, hypertension, third spacing Contraindication Hypersensitivity to sulfonamides, anuria, hypovolemia, infants, lactation and electrolyte depletion Drug Interaction >increased toxicity with lithium, non-depolarizing skeletal muscle relaxant >increased hypotensive action with antihypertensives and nitrates Side/Adverse Effects
>increased ototoxicity with aminoglycosides, cisplatin, vancomycin CNS: headache, fatigue, weakness, vertigo CV: orthostatic hypotension, chest pain, ECG changes circulatory collapse EENT: loss of hearing, ear pain, tinnitus and blurred vision ELECT: hypokalemia, hypochloremic alkalosis, hypocalcemia, matabolic alkalosis
GI: nausea, diarrhea, dry mouth, abdominal cramps, gastric irritaions GU: polyuria, renal failure, glycosuria HEMA: thrombocytopenia, agranulocytosis, anemia Nursing
INTEG: rash, pruritus, purpura, diaphoresis >assess for drowsiness and restlessness for it may indicate metabolic
Responsibilities alkalosis >monitor for signs of hypokalemia; postural hypotension, malaise, fatigue, tachycardia, leg cramps and weakness >observe hearing problems including tinnitus and hearing loss >monitor I & O qd to determine fluid loss. >monitor vital signs; rate, depth, and rhythm of respiration >ister in AM to avoid interference with sleep if using drug as diuretic > Use sterile equipment and apply principles of asepsis. > Ensure correct identification of the patient prior to the procedure. >Decontaminate hands prior to the procedure. >The cannula insertion site should be inspected for complications, i.e. infiltration, infection. >instruct patient to increase fluid intake 2-3 L/day unless contraindicated >tell the patient to rise slowly from lying or sitting position because orthostatic hypotension may occur >evaluate for therapeutic response
Generic Name Brand Name Photo
Omeprazole Losec and Prilosec
Classification Gastric acid secretion, proton-pump inhibitor Dosage and Route 40mg IVTTq12 Mechanism of Suppress gastric acid secretion by inhibiting the partial cell H+/K+ Action Indication Contraindication Drug Interaction
ATP pump To prevent ulceration in patients under NPO Known hypersensitivity to omeprazole decreased effect: decreased ketoconazole; decreased itriconazole increased toxicity: diazepam increase half-life; increased digoxin,
increased phenytoin, increased warfarin Side/Adverse EffectsCNS: headache, dizziness Neuromascular & Skeletal: weakness, back pain GI: nausea, diarrhea, vomiting, abdominal pain, constipation, taste perversion Nursing Responsibilities
Respiratory: upper respiratory infection, cough Ensure ten rights of medication istration Instruct patient not to chew, crush or open capsule Instruct patient to take before eating, capsule should be swallowed whole
Warn patients that Zegerid contains 460 mg sodium bicarbonate per dose. Those following a sodium-restricted diet should be cautious. Tell patient to empty contents of Zegerid packet into a small cup containing 2 tablespoons of water. Instruct patient to take drugs 30 minutes before meals. Caution patient to avoid hazardous activities if he gets dizzy. Inform patient that prilosec OTC may take 1-4 days for full effect.
Generic Name Brand Name Photo Classification
Spironolactone Aldactone Electrolyte and water balance agent; potassium sparing diuretic
Dosage and Route PO – (25, 50, 100) mg tablets
DOSING: Edema – 25 – 200 mg/d in divided doses, continued for atleast 5 daysd
Mechanism of
One of the main functions of the kidneys is to retain salt (sodium
Action
chloride) and water in the body. In patients with heart failure and cirrhosis, increased levels of a hormone produced by the adrenal glands, called aldosterone, causes salt and fluid to be retained by the kidneys. (At the same time, it also causes the kidneys to eliminate potassium.) The body becomes overloaded with salt and water, and this worsens the heart failure. Spironolactone inhibits the action of aldosterone thereby causing the kidneys to excrete salt and fluid in the urine while retaining potassium. Therefore, spironolactone is classified as a potassium-sparing diuretic, a drug that promotes the output of urine (diuretic) while allowing the kidneys to hold onto
Indication
potassium. clinical conditions associated with augmented aldosterone production, as in essential hypertension, refractory edema due to CHF, hepatic cirrhosis, nephritic syndrome and idiopathic edema
Contraindication Patients
with
anuria,
acute
renal
insufficiency,
significant
impairment of renal excretory function, or hyperkalemia. Drug Interaction Spironolactone can lower blood sodium levels while raising blood potassium levels. Excessively high blood potassium levels can lead to potentially life-threatening abnormalities in the rhythm of the heart. Therefore, spironolactone usually is not istered with
Generic Name
Ceftriaxone
Photo
Brand Name
Rocephin
Classification
cephalosporin antibiotic
Dosage and Route
1gm IVTTq12
Mechanism of
This antimicrobial agent inhibits bacterial cell wall synthesis by
Action
binding to one or more of the penicillin-binding proteins (PBPs) which in turn inhibits the final transpeptidation step of peptidoglycan synthesis in bacterial cell walls, thus inhibiting cell wall biosynthesis. Bacteria eventually lyse due to ongoing activity of cell wall autolytic enzymes (autolysins and murein hydrolases) while cell wall assembly is arrested.
Indication
Respiratory tract and intraabdominal infections
Contraindication
Cephalosporin hypersensitivity.
Drug Interaction
Warfarin (Coumadin, Jantoven) If you are taking ceftriaxone and warfarin, your body may metabolize the drugs differently than intended. You healthcare provider may choose to monitor your INR and prothrombin time more frequently and adjust accordingly. INR and prothrombin time are tests used to measure how well your blood clots.
Probenecid (Benemid, Probalan) If you are taking both ceftriaxone and probenecid, your body may metabolize the drugs differently than intended and significantly increase the amount of ceftriaxone in your system. Your healthcare provider may choose to monitor your progress
Generic Name
metronidazole
Photo
Brand Name
Flagyl
Classification
Anti-infectives, antiprotozoals, antiulcer agents
Dosage and Route Mechanism of Action
500mg 1 TAB q6 Disrupts DNA and protein synthesis susceptible organisms. Therapeutic effects: Bactericidal, trichomonacidal or amebicidal action. Spectrum: Most notable for activity against anaerobic bacteria including: Bacteroides, clostridium. In addition is active against: Trichomonas vaginalis, entamoeba histolytica, giardia lamdia, H. pylori and clostridium difficile.
Indication
PO: Amebecide in the management of amebic dysentery, amebic liver abscess and trichomoniasis: treatment of peptic ulcer disease caused by Helicobacter pylori.
Contraindication
Hypersensitivity. Use cautiously in: history in blood dyscrasias, History of seizures or neurologic problems and severe hepatic impairement.
Drug Interaction
Drug-drug: Cimetidine may decrease metabolism of metronidazole. Phenobarbital and rifampin increases metabolism and may decrease effectiveness. Metronidazole increases the effects of phenytoin, lithium, and warfarin. Disulfiram-like reaction may occur with alcohol ingestion. May cause acute psychosis and confusion with disulfiram. Increased risk of leucopenia with fluorourousel or azathioprine.
Side/Adverse Effects CNS: Seizures, dizziness, headache.
Generic Name
Lactulose
Photo
Brand Name
Contulose
Classification
Laxative
Dosage and Route
30cc @ bedtime
Mechanism of
Produces osmotic effect in colon. Resulting distention promotes
Action
peristalsis. Decrease blood ammonia build- up the causes hepatic encephalopathy, probably ass result of bacterial degradation which lowers pH of colon contents. Relieves constipation, decreases ammonia concentration.
Indication
- constipation - To prevent and treat hepatic encephalopathy, including hepatic precoma and coma I patients with severe hepatic disease. - to restore bowel movements after hemorrhoidectomy.
Contraindication
Contraindicated in patients on low- galactose diet
Drug Interaction
Drug-drug. - Should not be used with other laxatives in the treatment of hepatic encephalopathy - Anti- infectives may diminish effectiveness in treatment of hepatic encephalopathy
Side/Adverse Effects GI: belching, cramps, distention, flatulence, diarrhea ENDO: Hyperglycemia Nursing
Generic Name
Essentiale Forte
Photo
Brand Name
Essential Forte
Classification
Cholagogues, Cholelitholytics & Hepatic Protectors
Dosage and Route
1 cap TID
Mechanism of
Increase functional status of the liver, improvement in the lipids
Action
metabolism caused by accelerated synthesis of lipoproteins in the liver, activation of the phospholipid-depending ferments, increased synthesis of glycogen in the liver, decreased the fatty infiltration of the hepatocytes
Indication
- cirrhosis - Hepatic steatosis (also in cases of diabetes) - Acute and chronic hepatitis - Necrosis of the liver cells - Hepatic coma and precoma - Toxic liver damage (including pregnancy toxicosis)
Contraindication
- Contraindicated in patients hypersensitive to drug -in newborn children -in pregnant women
Drug Interaction
Not indicated
Side/Adverse Effects In very rare cases it can cause :abdominal pain, nausea, diarrhea and allergic reaction(skin rash). Nursing Responsibilities
1. Instruct patient on proper use of the drug
Generic Name
Phytonadione
Photo
Brand Name
Aqua-Mephyton, Vitamin K
Classification
Vitamin ( fat soluble)
Dosage and Route Mechanism of Action
1 amp now, OD -Required for hepatic synthesis of blood coagulation factors II (prothrombin), VII, IX, and X. - prevention of bleeding due to hypoprothrombinemia
Indication
•
Anticoagulant-induced prothrombin deficiency caused by coumarin or indanedione derivatives;
•
Prophylaxis and therapy of hemorrhagic disease of the newborn;
•
hypoprothrombinemia due to anti-bacterial therapy;
•
hypoprothrombinemia secondary to factors limiting absorption or synthesis of vitamin K, e.g., obstructive jaundice, biliary fistula, sprue, ulcerative coilitis, celiac disease, intestinal resection, cystic fibrosis of the pancreas, and regional enteritis;
•
Contraindication Drug Interaction
other drug-induced hypoprothrombinemia.
Hypersensitivity to any component of this medication. -Large doses will counteract the effect of warfarin - large doses of salicylates or broad-spectrum
Generic name
paracetamol
Photo
Brand name
Aeknin
Classification
Therapeutic: antipyretics, non-opiod analgesics
Ordered Dosage and
300mg IVTT now
Frequency Mode of Action
Inhibits the synthesis of prostaglandins that may serve as mediators of pain and fever, primarily in the CNS. Has no a significant anti-inflammatory property or GI toxicity. Therapeutic Effects: analgesia, antipyresis.
Indication
Mild pain, Fever
Contraindication
Contraindicated in: Previous hypersensitivity. Products containing alcohol, aspartame, saccharin, sugar, or tartrazine should be avoided in patients who have hypersensitivity or intolerance to these compounds. Used cautiously in: Hepatic disease/renal disease; chronic alcohol use/abuse; Malnutrition
Drug Interactions
Drug-drug: Chronic high-dose acetaminophen may increase the risk of bleeding with warfarin. Hepatoxicity is additive with other hapatotoxic substances, including alcohol.
Adverse Reactions/ Side Effects
GI: Hepatic failure, hepatoxicity (overdose) GU: renal failure(high doses/chronic use) Hemat: neutropenia, pancytopenia, leukopenia
Generic name
Tranexemic acid
Photo
Brand name
Cyclokapron
Classification
Hemostatic agent, antifibronolytic agent
Ordered Dosage and
100mg IVTT q8
Frequency Mode of Action
Inhibits activation of plasminogen, thereby preventing the conversion of plasminogen to plasmin
Indication
Prevention of hemorrhage
Contraindication
Hypersensitivity, active intravascular clotting
Drug Interactions
Concurrent use of clotting factor, complexes may increase the risk of thrombotic complications. risk of thrombosis may be increased by estrogens. Drug will antagonize the effects of thrombolytic agents.
Adverse Reactions/ Side Effects
CNS: visual abnormalities CV: hypotension, thrombosis, thromboembolism GI: nausea, vomiting, diarrhea
Nursing
i.
Responsibilities
observe the 10 rights of medication istration of medication
ii.
check for hypersensitivity to drug
iii.
observe for bleeding
iv.
instruct patient ot take tranexamic acid as directed
NURSING THEORIES
Theorist: Dorothea Orem Theory: Self-care Deficit Theory Orem’s theory states that each person has a need for self care in order to maintain optimal health and wellness. Each person possesses the ability and responsibility to care for themselves and dependants. The theory is separated into three conceptual theories which include: self-care, self-care deficit, and nursing system. Self care is the ability to perform activities and meet personal needs with the goal of maintaining health and wellness of mind, body and spirit. Self-care is a learned behavior influenced by the metaparadigm of person, environment, health and nursing. There are three components of this theory: universal self-care needs, developmental self-care needs, and health deviation. Universal theory includes activities which are essential to health and vitality. Developmental self-care need include the interventions and teachings designed to return to a person to or sustain a level of optimal health and well-being. Health Deviation selfcare encomes the variation of meeting self-care which may occur as a result of disability, illness or injury. Orem created three areas of how care can be istrated to a client depending on the physical and mental capabilities of the client: the wholly compensatory, partly compensatory and the ive-educative role. The wholly compensatory system accomplishes the client’s therapeutic self-care, compensates for the client’s inability to participate in their self-care, provides and protects the client. The partly compensatory is a give and take system between the client and the nurse. The nurse performs, compensates and assists the client as needed while the client participates,
regulates and accepts care and assistance form the nurse. Lastly, the ive-educative role indicates that the client is participating in most of their self-care, and the nurse’s role is simply to monitor and regulate the client’s self-care.
Application to client: The client’s environment failed to provide adequate warmth and ventilation. It has a limited space and is not quiet enough for the client to take adequate rest. These factors contributed to the client’s present condition as well as his ability to cope and recover. The nurse’s role is to help client achieve optimal health and wellness by acting as an advocate, redirector, person and teacher and to provide an environment conducive to therapeutic development. One example of this theory is by creating nursing care plans which was made by the student nurses. The theory applies to the assessment and evaluation of the nursing process. Since patient is in a comatose state, we have applied the wholly compensatory system. Since patient is unable to do the self-care activities, the nurse together with the medical team assisted the client’s needs by providing adequate care to the patient through helping the client achieve good hygiene, preventing bed sore by turning the patient to sides, preventing injury and promoting rest and comfort to the patient. Also, nurses were able to create nursing care plans which became their guide on how to render care to the patient. Also, important health teachings were provided to the family of the patient.
Theorist: Lydia Hall Theory: Core, Care and Cure Theory Hall's theory emphasizes the importance of individuals as unique, capable of growth and learning, and requiring a total person approach. Her definition of health can be inferred to a state of self-awareness with conscious selection of behaviors that are optimal for that individual. Hall stresses the need to help the person explore the meaning of his or her behavior to identify and overcome problems through developing self-identity and maturity. The concept of society or environment is dealt with in relation to the individual. Hall's theory of nursing involves three interlocking circles, each one of it represents one aspect of nursing. The same aspect represents intimate bodily care of the patient. The core aspect deals with the innermost feeling and motivations of the patient and family through the medical aspects of care. Care is the sole function of nurses, where as core and cure are shared with other of the health care team. The major purpose of care is to achieve interpersonal relationship with the individual. The nurse plans and prepares a series of independent nursing interventions that can aid from its condition. These interventions are designed to provide good and conducive atmosphere, istering drugs to the right patient, right drug and right time. The nurse also provides health teachings to the client’s family on medication management and independent actions such as advising the client to have complete bed rest.
Theorist: Faye Glenn Abdellah Theory: Twenty-one Nusring Problems Abdellah’s theory would state that nursing is the use of the problem solving approach with key nursing problems related to health needs of people. Such a statement maintains problem solving as the vehicle for the nursing problems as the client is moved toward health – the outcome. Faye Abdellah formulated the twenty-one Nursing Problems and categorizes them into three: the Physical, sociological, and emotional needs of clients, the types of interpersonal relationships between the nurse and patient and the common elements of client care. The 21 Nursing Problems were divided into four care needs: Basic to all patients, Sustenal care needs, Remedial care needs and Restorative care needs. The Nursing problem presented by a client is a condition faced by the client or client’s family that the nurse through the performance of professional functions can assist them to meet. An overt nursing problem is an apparent condition faced by the patient or family, which the nurse can assist him or them to meet through the performance of her professional functions. The covert nursing problem is a concealed or hidden condition faced, by the patient or family, which the nurse can assist him or them to meet through
the performance of her professional functions. According to Abdellah, nursing is a helping profession.
Application to Client: Since our patient is suffering from his condition, the student nurses have identified nursing problems which made them choose the theory of Abdellah. The patient was in a state of coma and so he was not able to perform certain activities which he needs. Thus, student nurses provided care and assisted the client and his family. Some of the nursing interventions done to address the problems identified by the student nurses which falls under the 21 nursing problems theory were: maintained good hygiene and physical comfort, promoted rest and sleep, promoted safety through the prevention of accidents, injury, or other trauma and through the prevention of the spread of infection, maintained good body mechanics and prevent and correct deformity, To facilitate the maintenance of a supply of oxygen to all body cells, facilitated the maintenance of elimination, recognize the physiological responses of the body to disease conditions, created and / or maintained a therapeutic environment. The student nurses focused their interventions to the needs of the patient which helps in the promotion of recovery to the patient.
NURSING CARE PLANS Date / Time
Cues
February
Objective:
A
- crackles
C
11, 2010 at 4pm
heard on lung field upon ausculatation -with bag valve connected to endotracheal tube
Needs
T I
Nursing Diagnosis
Ineffective airway
At the end of
clearance related to
7 hours span
accumulation of
of care, the
secretions secondary
patient will
to Community
have
Acquired Pneumonia
effective
V I T Y E X E
Objective of Care
airway as evidenced by R: Pneumonia, which
absence of
is an acute infection
crackles.
of the lungs, causes inflammation in lung tissues which leads to
Nursing Intervention
1. Provide suctioning. R: to clear airway from accumulated
Evaluation
February 11, 2010; 11pm
secretions.
GOAL UNMET
2. Elevate head of bed.
After rendering
R: Gravity decreases pressure on the diaphragm 3. Turn patient to sides every 2 hours R: repositiong enhances drainage and promotes ventilation to different lung segments.
nursing interventions within the 7hours span of care, the patient has still ineffective airway clearance
damage on mucous
4. Assist in providing respiratory
as evidenced by
and alveolar
through ambu bagging.
presence of
membranes. This damage results in secretion of exudates and mucous as the
R: mechanical ventilation maintains adequate airways and improve respiratory functions.
crackles on lung field.
R C I S
system tries to get rid with the infection. This secretions cause obstruction in the airway.
A T T E R N
R: to maintain anatomic position of the tongue and provide natural airway 6. Re-ausculate lung sound R: to note for progress, if crackles are
E P
5. Insert mouth guard.
Williams, L.S &
still present.
Hoppers, P.D. (2007).
7. Provide oxygen with appropriate
Understanding
humidifier, as ordered.
medical-surgical nursing,3rd ed. Philadelphia: F.A. Davis Company.
R: to facilitate oxygenation and liquefy secretion for easy suctioning. 8. Monitor oxygen saturation. R: to rule out presence of gas exchange impairement. 9. Carry out diagnostic orders made by the physician such as ABG or AFB and secure result. R: to determine the degree of respiratory impairment such as
presence of hypoxemia.
Date
Cues
Needs
Nursing. Diagnosis
F
Objective cues:
N
Bleeding related to altered
E B R
-
Melena
noted Decreas
U
-
A
ed platelet
R
count of 115
Y
x103 /uL (Normal:
11,
150-400
2010
x103 /uL)
@ 5:00 PM
-
Gastric
lavage ordered
U T R I T I O N A L
Intervention
Evaluation
Within the 8
1. Monitor patient’s vital
February 11, 2010
clotting mechanism:
hours span of
signs, especially the
decreased prothrombin and
care, the patient
blood pressure
thrombin production
will be able to:
secondary to liver cirrhosis
M E
® To obtain baseline
maintain normal
data and prevent
® One of the functions of
hemodynamic
hypotension
liver is the production of
status as
prothrombin and thrombin
evidenced by a
which are substances
normal intake
needed to help blood
and output
2. Assess patient’s level of consciousness ® A change in the level
coagulate. In patients with
of consciousness
liver cirrhosis, they are at
indicates a decrease in
higher instances of
circulating blood volume
bleeding because of the decreased coagulation factors.
-
Objective
3. Monitor intake and output ® To determine fluid balance and prevent dehydration 4. Regulate intravenous
T
fluids appropriately
A
® To prevent
B
dehydration and correct the normal
O
hemodynamic status
L
5. Monitor hematocrit and
@ 10:30 PM Goal Met Within the 8 hours span of care, the patient was able to maintain normal hemodynamic status as evidenced by a normal intake and output
Date /Time February
Cues Objective Cue:
Nursing Diagnosis
Objective/Goal
Intervention
N
Hyperthermia related to the
Within my 1-3 hour
1.
U
release of endogenous
span of care, my
signs.
- Increased
T
pyrogen secondary to
patient’s body
® serves as baseline data
body
R
presence of CAP and liver
temperature will
temperature of
I
cirrhosis
decrease from 38.1°C
2.
38.3
T
to 36.5-37.5°C.
developmental age of client.
11, 2010 5:00pm
Needs
Monitor patient’s vital
@ Note chronological and
R: Hyperthermia is the
® Elderly or impaired
O
elevation of body temperature
individuals ay not be able to
is warm to
N
above normal range. Most
recognize and/or act on
touch
A
often, it results from infection
symptoms of hyperthermia
L
somewhere i the body, but it
-
Skin
Increa
sed
diagnos
is of CAP
GOAL MET Patient’s body temperature
3.
conditions (cancer, allergic
bath
from 38.1 ° C
reactions, and CNS injuries).
® promotes heat loss by
to 36.7° C
M
Macrophages, white blood
evaporation and conduction
E
cells, and injured cells release
T
chemical substances called
4.
A
pyrogens that act directly on
lightweight, loose-fitting
B
the hypothalamus, causing its
clothes.
O
thermostat to be set to a
® encourages heat loss by
respiratory
-
8:00pm
may be caused by other -
rate of 24
February 11, 2010
I -
Evaluation
Provide tepid sponge
Limit clothing in
decreased
-
ascites
L
higher temperature.
radiation and conduction.
Reference:
5.
Nurse’s Pocket Guide 10th
with air-conditioning or fans.
Edition by Doenges, et al.
® promotes heat loss by
I C P A
Cool the environment
convection
T T
6.
Keep clothing and linens
E
dry.
R
® to reduce shivering
N 7.
ister replacement
fluids and electrolytes ® to replace fluids lost through perspiration and respiration. 8.
Maintain bedrest
® to reduce metabolic demands 9. Discuss importance of adequate fluid intake
® To prevent dehydration INTERDEPENDENT 10.
Collaborate with
dietician in providing patient with high-calorie diet, or parenteral nutrition ® to meet increased metabolic demands 11.
Notify physician if
pharmacologic regimen is inadequate to meet hyperthermia control goal. ® to determine if there is a need to increase dosage, change medication or use a stepped program (e.g., switching from injection to oral route, or lengthening time interval between doses).
DEPENDENT 12.
ister antipyretics,
orally or rectally, as ordered. ® to aid in reducing the body temperature 13.
Provide supplemental
oxygen as ordered. ® to offset increased oxygen demands and consumption. 14.
ister replacement
IV fluids and electrolytes as ordered. ® to circulating volume and tissue perfusion and to aid in hydration
DATE/ CUES
NEE
NURSING
OBJECTIVES OF
D
DIAGNOSIS
CARE
TIME F
Objective:
E B R U A
N - ascites -dry, scaly and shiny -edema
R Y
U T R I T
-dyspnea
I O
1
N
1
A
,
L -
Fluid
Within 8 hours span
Volume
of care, the client
Excess in the
will be able to :
NURSING INTERVENTIONS
1.
® To obtain baseline date and
space related to liver organ
a. Stabilize
failure as
fluid volume as
evidenced by
evidenced by
2.
ascites
balanced I/O,
dependent venous pooling or
with liver failure, there is a decreased
Vital signs within normal limits
venostasis. ® To determine causative factors 3.
Thus,
environment, limiting external
osmotic
Provide quiet
stimuli. ® To promote adequate rest
2
M
pressure in
0
E
the
and comfort for faster
intravascular
recovery
1
T
spaces. This
0
A
leads to the
4.
Monitor intake and output
accumulation @
B
of fluid in the
Goal Unmet
Assess for evidence of
albumin.
decrease in
11:00 pm
to note any unusualities
production of
resulting to
February 11, 2010
Measure vital signs
@
interstitial
®In patients
EVALUATION
® To determine elimination o
Patient was unable to: o
stabilize fluid volume as evidenced by imbalance intake and output
Date / Time
Cues
February
Objective:
N
-
U
11, 2010 at
Needs
Nursing Diagnosis w/ Rationale
4pm
Jaundice noted in the skin upon inspection .
-
+4 pitting edema noted on all four extremitie
T R I T I O N
s -
(+) body malaise
A
Risk for impaired
Within my
skin integrity related
seven hours
to prolonged bed rest
span of care,
R: When edema and jaundice are present, the skin is placed at more risk of being
the patient will maintain undamaged physical
impaired because of
Skin integrity
the bilirubin present
by not
on the blood.
manifesting
Moreover, prolonged bed rest can form decubitus ulcers at the patient’s back.
L
Vital Signs: BP- 110/70
Objective of Care
signs of decubitus ulcer.
Nursing Intervention w/ Rationale 1. Monitor patient’s vital signs. ® serves as baseline data
February 11, 2010; 10pm
2.) Assess for any changes in skin. ® to be able to determine the causative factors 3.) Note and record degree of jaundice of skin and sclera and scratches on the body. ® to be able to assess skin integrity 4.) Maintain strict skin hygiene.
Goal Met: After seven hours span of care, the patient still maintained intact skin integrity as evidenced by absence of
® to prevent the spread of bacteria
decubitus ulcer
and prevent infection
at the patient’s
5.) Provide adequate clothing/covers. Reference :
Evaluation
®to prevent vasoconstriction
back.
mmHg
M
PR- 96 bpm
E
RR- 24 cycles
T
per minute TEMP. – 38.3 °C
Nurse’s Pocket Guide
6.) Observe for reddened/blanched
11th Edition by
areas and institute treatment
Doenges, et al.
immediately. ®: Reduces likelihood of progression
A
to skin breakdown.
B
7.) Change patient’s position every
O L I C
two hours. ®: To relieve the pressure on the patient’s back. 8.) Drain urine bag every two hours. To monitor output of patient in order to determine fluid and electrolyte
P A T T E
intake and loses 9.) Encourage frequent skin care to significant other. Also, perform morning care to patient by performing complete bed bath and apply lotion afterwards. ®: To promote hygiene and skin
R N
integrity. To promote skin moisture, and prevent roughness on skin. 10.) Emphasize importance of adequate nutritional/fluid intake to significant others. (through NGT feeding) ®: to maintain general good health and skin turgor. 11.) ister medications as ordered. ® to treat any underlying cause
POST-MORTEM
Ask permission to the family before doing the post-mortem care.
R: The family is in grieving stage and so nurses should be sensitive enough in dong responsibilities
Ask permission to the patient before removing tubing from his body
R: It is to convey respect and value to the patient’s body
Use caution when removing tape from the body to avoid skin breakdown.
R: The body temperature decreases with a resultant lack of skin elasticity
Elevate the head to prevent discoloration from the pooling of blood.
R: a physiological change will happen in which a bluish purple discoloration that is a by-product of red blood cell destruction occurs in the dependent areas in the body.
The nurse should close the eyelids, insert dentures, close the mouth and position the body in a natural position as soon as possible after death.
R: To prevent the body from stiffening caused by contraction of skeletal and smooth muscles.
Prepare the body: remove all tubes and position the body
R: To make the body look comfortable and natural for family viewing.
Place the body in a plastic or fabric shroud and put a tag on it.
R: To prepare the body for transport to the morgue.
Return the deceased’s possession to the family such as jewelries, eyeglasses, clothing and all personal items.
Offer to people
Help the family with decision making regarding funeral home, transportation, and the removal of the deceased’s belongings.
R: The family needs help since they are on the process of grieving.
Demonstrate comion in providing information and to families.
R: This will inform the family of your genuine concern for them
PROGNOSIS
Criteria Onset of Illness
Poor
Fair
Good
Justification We rated it poor since the
patient started manifesting symptoms that are associated with liver cirrhosis since December 2009. On January 23, 2010, 13 days prior to his ission, the patient experienced headache, chest pain, dull abdominal pain, felt nauseated and dizzy.. Duration of
Occurrence of
Illness
manifestations related to liver cirrhosis has been observed to start since December 2009. It is also poor since liver cirrhosis is a chronic disease. Hospital days until our last with the patient are 6 days.
Attitude and
As verbalized by his wife,
willingness to
the patient is taking
take
medications but sometimes
medications
with skipped doses because he neglects to take and due to forgetfulness.
Age
The patient is 73 years old and we rated it as poor since geriatric patients have deteriorating body systems that hinder recovery. The wear and tear theory suggests that as a person ages, he or she is more prone to illness and resistance and the ability to heal is getting weaker.
Precipitating
We rated it poor since his
and
age and race predisposes
predisposing
him in developing the
factors
disease. Moreover, his chronic alcoholism precipitates the development of the disease. Longtime alcohol beverage drinking is
the most common factor that triggers liver cirrhosis. Environment
The ward has poor
ventilation, crowded and noisy. With this, it is not favorable for recovery. Family
Family is fair. They give time in giving care to the patient but cannot provide all the needs especially the medications and mechanical ventilator because of financial inadequacy.
Basis for Prognosis: Poor = 1
Fair = 2
Good = 3
Range of prognosis: 0-1.50 = poor 1.51-2.0 = fair 2.0-2.5 = good
Result: POOR: Precipitating and predisposing factors, Age, Duration of Illness, Onset of Illness, Environment FAIR: Attitude and willingness to take medications and Family GOOD: None
Computation: Good: 3 x 0 = 0 Fair: 2 x 2 = 4 Poor: 1 x 5 = 5 Total: 9/7 = 1.28 (POOR PROGNOSIS)
RECOMMENDATION Every rotation we have is a learning course and practice to develop our skills and hearts as caregivers. In this rotation, the 3rd group of BSN-3H, cultured a lot of knowledge in this experience; experience that will serve as our guide and basis for improvement. In relation with improvement, the group had come up with recommendations, which we think, would have made the exposure a lot better. To our client’s family: One of the most important factors of recovery for a certain illness is the participation of the patient himself. However, our client has suffered a disease wherein he has gone seriously affected both physically and emotionally and even his consciousness and responsiveness have been depleted. The family’s involvement in the treatment of the patient is very essential and highly needed. The family should know all the basic facts and information about the patient’s illness because them, more than anybody else are expected not just to care but also to accept his condition with utmost understanding. Being aware of the illness itself and its treatment will elicit awareness and would definitely pave the way to the prevention and alleviation of any ailment that any of the family may possibly have. To the family , the death of a love one is not the end of every one’s life. His death should serve a lesson and be a step towards taking good care of one’s body.
To the Student Nurses: In line with this case study, the group would like to encourage all student nurses to get more involved in the promotion of health in our country. We are to provide health services to the greater population in a way that it is more generalized. We must impart to those who are in need, our knowledge regarding health and on how they could maintain a healthy lifestyle. We must apply to them the skills that we have learned by rendering them a quality- based service. We must also teach the patients as well as the significant others on the alternative means of promoting health and on how to prevent the possible occurrence of a disease. Empathy must always be shown not just to the patient but also to the significant others. Student nurses must also be sensitive to the feelings and emotions not just of the patient but also to the significant others especially in experiences of death and finite separation. To the medical world:
We would like to encourage the medical practitioners or the of the health care team that they should have to be more committed or comionate in their chosen profession. They must have to cater the health needs of the people of different kinds without putting levels of discrimination on them. Their job is not that easy but they must have to be very careful because they are already dealing here with the life of a person. They must have to extend their hands not only in the physical means but also in a holistic way of giving or providing care to individuals, families and the population groups especially in significant others who may have lost love ones.. They are tasked to render
their services in order to achieve the good health condition of the citizens of the country because the health of the nation lies in the health of the populace.
REFERENCES
BLACKWELL’S DICTIONARY OF NURSING 5TH EDITION, 2004 BROWN, K.S (2003) DEVELOPMENTAL THEORY: UNDERSTANDING THE AGES. RETRIEVED FROM HTTP://WWW.HAVERFORD.EDU/PSYCH/DDAVIS/P109G ERIKSON.STAGES.HTML. RETRIEVED ON FEBRUARY
12, 2010.
HANDBOOK OF MEDICAL-SURGICAL NURSING 3RD ED. SPRINGHOUSE: 2006 LEIGHTON, S.S., ET AL.(1997) PERSPECTIVE IN HUMAN DEVELOPMENT. RETRIEVED FROM HTTP://WWW.SLIDESHARE.NET/SUNNYCUTS/JEAN-PIAGETS-THEORIES-OF-DEVELOPMENT. RETRIEVED ON FEBRUARY 20, 2010. LINDON, P.S & REESE, R.R. ( 1999) PSYCHOLOGY: APPROACH AND UNDERSTANDING. RETRIEVED FROM HTTP://PSYCHOLOGY.ABOUT.COM/OD/THEORIESOFPERSONA LITY /A/PSYCHOSOCIAL_3 .HTM. RETRIEVED ON
FEBRUARY 12, 2010.
LINDON, P.S & REESE, R.R. ( 1999) PSYCHOLOGY: APPROACH AND UNDERSTANDING. RETRIEVED FROM HTTP://EDUCATION.STATEUNIVERSITY.COM/PAGES/2032/HAVIGHURST-ROBERT-J-19001991.HTML. RETRIEVED ON FEBRUARY 12, 2010. LUCKMANN, K.L & SORENSEN, W.A (2003) : MEDICAL-SURGICAL NURSING: A PSYCHOPHYSIOLOGIC APPROACH. LOUIS, MISSOURI: MOSBY. MCTIMOTHY, A.S (2005) PATHOPHYSIOLOGY: A 2-IN-1 REFERENCE FOR NURSES. PHILADELPHIA: LIPPINCOTT WILLIAMS & WILKINS. PETERSON, M.L, LUIS, B.D. & CHONG, P.C.(2000)PERSONALITY DEVELOPMENT. RETRIEVED FROM HTTP://BAMA.UA.EDU/~JSTALLWO/YAL/ARTICLES/YOUNG%20ADULT%20LITERATURE%20IN %2 0THE%20CLASSROOM.PDF. RETRIEVED ON FEBRUARY 22, 2010.
REYBURN, S. W. (2001) MANUAL OF MEDICAL EDUCATION. RETRIEVEDFROM HTTP://WWW .AAFP.ORG/AFP /2006/0201/P44 2.HTML ACCESSED ON FEBRUARY 21, 2010 SUDDARTH, D.R. (1991) THE LIPPINCOTT MANUAL OF NURSING PRACTICE, 5TH ED. PHILADELPHIA: LIPPINCOTT WILLIAMS & WILKINS. WONG, L.D. (2000) UNDERSTANDING LIVER CIRRHOSIS. RETRIEVED FROM HTTP://WWW.EMEDICINEHEALTH.COM/CIRRHOSIS/PAGE2_EM.HTM#CIRRHOSIS%20CAUSES.
RETRIEVED ON FEBRUARY 22, 2010.
Related Documents c2h70
Liver Cirrhosis Case Presentation 4r423w
April 2022 0
Liver Cirrhosis Case Presentation 4r423w
October 2019 160
Liver Cirrhosis Case Pres 6u4g8
December 2019 71
Liver Cirrhosis Case 3rb63
December 2021 0
Case Study Liver Cirrhosis 5b322w
December 2021 0