Interact Sbar Form 3oa3o
This document was ed by and they confirmed that they have the permission to share it. If you are author or own the copyright of this book, please report to us by using this report form. Report 2z6p3t
Overview 5o1f4z
& View Interact Sbar Form as PDF for free.
More details 6z3438
- Words: 756
- Pages: 3
SBAR Communication Form and Progress Note
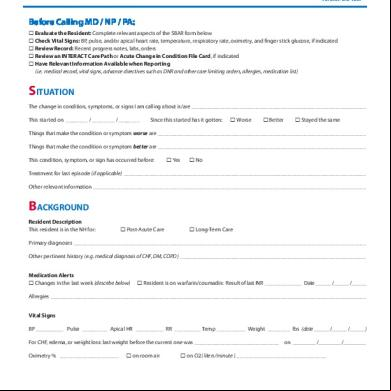
Before Calling MD / NP / PA: Evaluate the Resident: Complete relevant aspects of the SBAR form below Check Vital Signs: BP, pulse, and/or apical heart rate, temperature, respiratory rate, oximetry, and finger stick glucose, if indicated Review Record: Recent progress notes, labs, orders Review an INTERACT Care Path or Acute Change in Condition File Card, if indicated H ave Relevant Information Available when Reporting (i.e. medical record, vital signs, advance directives such as DNR and other care limiting orders, allergies, medication list)
SITUATION The change in condition, symptoms, or signs I am calling about is/are_______________________________________________________________ This started on ________ / ________ / ________
Since this started has it gotten:
Worse
Better
Stayed the same
Things that make the condition or symptom worse are___________________________________________________________________________ Things that make the condition or symptom better are___________________________________________________________________________ This condition, symptom, or sign has occurred before:
Yes
No
Treatment for last episode (if applicable)_______________________________________________________________________________________ Other relevant information__________________________________________________________________________________________________
BACKGROUND Resident Description This resident is in the NH for:
Post-Acute Care
Long-Term Care
Primary diagnoses_________________________________________________________________________________________________________ Other pertinent history (e.g. medical diagnosis of CHF, DM, COPD)___________________________________________________________________ Medication Alerts Changes in the last week (describe below)
Resident is on warfarin/coumadin: Result of last INR______________ Date ______ /______ /______
Allergies_________________________________________________________________________________________________________________ Vital Signs BP____________ Pulse__________ Apical HR ___________ RR __________ Temp___________ Weight _________ lbs (date ______ /______ /______ ) For CHF, edema, or weight loss: last weight before the current one was_______________________________ on _________ /_________ /_________ Oximetry % ______________________
on room air
on O2 ( liters/minute )_________________________________
Residents Name_______________________________________________________________________________________________________ (continued) ©2011 Florida Atlantic University, all rights reserved. This document is available for clinical use, but may not be resold or incorporated in software without permission of Florida Atlantic University.
SBAR Communication Form and Progress Note (cont’d)
For the next 5 items, complete only those relevant to the change in condition. If the item is not relevant, check ‘N/A’ for not applicable. 1. Mental Status Changes (compared to baseline; check all that you observe) N/A Increased confusion New or worsening behavioral symptoms Decreased consciousness (sleepy, lethargic) Unresponsiveness O ther symptoms or signs of delirium (e.g. inability to pay attention, disorganized thinking) Describe symptoms or signs _______________________________________________________________________________________________ 2. Functional Status Changes (compared to baseline; check all that you observe) Needs more assistance with ADLs Decreased mobility Weakness or hemiparesis Slurred speech
N/A Fall Trouble swallowing
Other (describe)
Describe symptoms or signs _______________________________________________________________________________________________ 3. Respiratory N/A Shortness of breath Abnormal lung sounds
Cough ( Non-productive Productive ) Labored breathing
Describe symptoms or signs _______________________________________________________________________________________________ 4. GI/Abdomen N/A Nausea Distended abdomen
Vomiting Tenderness
Diarrhea Decreased appetite Abdominal pain Decreased bowel sounds (date of last BM _______ / _______ / _______ )
Describe symptoms or signs _______________________________________________________________________________________________ 5. GU/Urine Changes (compared to baseline; check all that you observe) Decreased urine output Painful urination Needs to urinate more urgently Blood in urine
N/A Urinating more frequently New or worsening incontinence
Describe symptoms or signs _______________________________________________________________________________________________
Recent Lab Results (e.g. CBC, chemistry or metabolic , drug levels) ________________________________________________________________________________________________________________________ ________________________________________________________________________________________________________________________ Advance Care Planning Information (the resident has orders for the following advance directives) DNR DNI (Do Not Intubate) DNH (Do Not Hospitalize) No Enteral Feeding
Other Order or Living Will (specify)
________________________________________________________________________________________________________________________ Other resident or family preferences for care __________________________________________________________________________________________
Residents Name_______________________________________________________________________________________________________ (continued) ©2011 Florida Atlantic University, all rights reserved.
SBAR Communication Form and Progress Note (cont’d)
ASSESSMENT (RN) OR APPEARANCE (LPN) What do you think is going on with the resident? For RNs: I think the problem may be (e.g. cardiac, infection, respiratory, dehydration ) ___________________________________________________ ________________________________________________________________________________________________________________________ For LPNs: The resident appears (e.g. short of breath, in pain, more confused) __________________________________________________________ ________________________________________________________________________________________________________________________
REQUEST I suggest or request (check all that apply) Monitor vital signs Lab work X-ray Transfer to the hospital (send a copy of this form)
EKG Provider visit (MD/NP/PA) Other new orders (specify)
Nursing Notes (for additional information on the Change in Condition) ________________________________________________________________________________________________________________________ ________________________________________________________________________________________________________________________ ________________________________________________________________________________________________________________________ ________________________________________________________________________________________________________________________ ________________________________________________________________________________________________________________________ ________________________________________________________________________________________________________________________ ________________________________________________________________________________________________________________________ ________________________________________________________________________________________________________________________ ________________________________________________________________________________________________________________________ ________________________________________________________________________________________________________________________
Name of Family/Health Care Agent Notified:__________________________________________ Date ____ /____ /____ Time (am/pm)_________ Reported to Primary Care Clinician (MD/NP/PA):______________________________________ Date ____ /____ /____ Time (am/pm)_________
Staff Name (RN/LPN) and Signature__________________________________________________________________________________ Residents Name_______________________________________________________________________________________________________
©2011 Florida Atlantic University, all rights reserved.
Before Calling MD / NP / PA: Evaluate the Resident: Complete relevant aspects of the SBAR form below Check Vital Signs: BP, pulse, and/or apical heart rate, temperature, respiratory rate, oximetry, and finger stick glucose, if indicated Review Record: Recent progress notes, labs, orders Review an INTERACT Care Path or Acute Change in Condition File Card, if indicated H ave Relevant Information Available when Reporting (i.e. medical record, vital signs, advance directives such as DNR and other care limiting orders, allergies, medication list)
SITUATION The change in condition, symptoms, or signs I am calling about is/are_______________________________________________________________ This started on ________ / ________ / ________
Since this started has it gotten:
Worse
Better
Stayed the same
Things that make the condition or symptom worse are___________________________________________________________________________ Things that make the condition or symptom better are___________________________________________________________________________ This condition, symptom, or sign has occurred before:
Yes
No
Treatment for last episode (if applicable)_______________________________________________________________________________________ Other relevant information__________________________________________________________________________________________________
BACKGROUND Resident Description This resident is in the NH for:
Post-Acute Care
Long-Term Care
Primary diagnoses_________________________________________________________________________________________________________ Other pertinent history (e.g. medical diagnosis of CHF, DM, COPD)___________________________________________________________________ Medication Alerts Changes in the last week (describe below)
Resident is on warfarin/coumadin: Result of last INR______________ Date ______ /______ /______
Allergies_________________________________________________________________________________________________________________ Vital Signs BP____________ Pulse__________ Apical HR ___________ RR __________ Temp___________ Weight _________ lbs (date ______ /______ /______ ) For CHF, edema, or weight loss: last weight before the current one was_______________________________ on _________ /_________ /_________ Oximetry % ______________________
on room air
on O2 ( liters/minute )_________________________________
Residents Name_______________________________________________________________________________________________________ (continued) ©2011 Florida Atlantic University, all rights reserved. This document is available for clinical use, but may not be resold or incorporated in software without permission of Florida Atlantic University.
SBAR Communication Form and Progress Note (cont’d)
For the next 5 items, complete only those relevant to the change in condition. If the item is not relevant, check ‘N/A’ for not applicable. 1. Mental Status Changes (compared to baseline; check all that you observe) N/A Increased confusion New or worsening behavioral symptoms Decreased consciousness (sleepy, lethargic) Unresponsiveness O ther symptoms or signs of delirium (e.g. inability to pay attention, disorganized thinking) Describe symptoms or signs _______________________________________________________________________________________________ 2. Functional Status Changes (compared to baseline; check all that you observe) Needs more assistance with ADLs Decreased mobility Weakness or hemiparesis Slurred speech
N/A Fall Trouble swallowing
Other (describe)
Describe symptoms or signs _______________________________________________________________________________________________ 3. Respiratory N/A Shortness of breath Abnormal lung sounds
Cough ( Non-productive Productive ) Labored breathing
Describe symptoms or signs _______________________________________________________________________________________________ 4. GI/Abdomen N/A Nausea Distended abdomen
Vomiting Tenderness
Diarrhea Decreased appetite Abdominal pain Decreased bowel sounds (date of last BM _______ / _______ / _______ )
Describe symptoms or signs _______________________________________________________________________________________________ 5. GU/Urine Changes (compared to baseline; check all that you observe) Decreased urine output Painful urination Needs to urinate more urgently Blood in urine
N/A Urinating more frequently New or worsening incontinence
Describe symptoms or signs _______________________________________________________________________________________________
Recent Lab Results (e.g. CBC, chemistry or metabolic , drug levels) ________________________________________________________________________________________________________________________ ________________________________________________________________________________________________________________________ Advance Care Planning Information (the resident has orders for the following advance directives) DNR DNI (Do Not Intubate) DNH (Do Not Hospitalize) No Enteral Feeding
Other Order or Living Will (specify)
________________________________________________________________________________________________________________________ Other resident or family preferences for care __________________________________________________________________________________________
Residents Name_______________________________________________________________________________________________________ (continued) ©2011 Florida Atlantic University, all rights reserved.
SBAR Communication Form and Progress Note (cont’d)
ASSESSMENT (RN) OR APPEARANCE (LPN) What do you think is going on with the resident? For RNs: I think the problem may be (e.g. cardiac, infection, respiratory, dehydration ) ___________________________________________________ ________________________________________________________________________________________________________________________ For LPNs: The resident appears (e.g. short of breath, in pain, more confused) __________________________________________________________ ________________________________________________________________________________________________________________________
REQUEST I suggest or request (check all that apply) Monitor vital signs Lab work X-ray Transfer to the hospital (send a copy of this form)
EKG Provider visit (MD/NP/PA) Other new orders (specify)
Nursing Notes (for additional information on the Change in Condition) ________________________________________________________________________________________________________________________ ________________________________________________________________________________________________________________________ ________________________________________________________________________________________________________________________ ________________________________________________________________________________________________________________________ ________________________________________________________________________________________________________________________ ________________________________________________________________________________________________________________________ ________________________________________________________________________________________________________________________ ________________________________________________________________________________________________________________________ ________________________________________________________________________________________________________________________ ________________________________________________________________________________________________________________________
Name of Family/Health Care Agent Notified:__________________________________________ Date ____ /____ /____ Time (am/pm)_________ Reported to Primary Care Clinician (MD/NP/PA):______________________________________ Date ____ /____ /____ Time (am/pm)_________
Staff Name (RN/LPN) and Signature__________________________________________________________________________________ Residents Name_______________________________________________________________________________________________________
©2011 Florida Atlantic University, all rights reserved.
Related Documents c2h70
Interact Sbar Form 3oa3o
November 2019 85
Interact hip Application Form 282q47
December 2021 0
Form Komunikasi Metode Sbar 643870
April 2020 20
Sbar 2j1955
October 2020 0
Sbar 2j1955
December 2020 0
Manual Interact 70355t
February 2021 0More Documents from "Tisa Meriel" 4g641k
Interact Sbar Form 3oa3o
November 2019 85
1.sk Pembentukan Tim Dots 6o2y49
July 2020 1
Comparison En 10277 s362z
August 2021 0
Flupec Overview Hawe V30d 2t1731
June 2022 0
Teori Keperawatan Menurut Medeleine Leininger 6p4k37
April 2020 19