Forensic Mnemonics - Metals 4h1de
This document was ed by and they confirmed that they have the permission to share it. If you are author or own the copyright of this book, please report to us by using this report form. Report 2z6p3t
Overview 5o1f4z
& View Forensic Mnemonics - Metals as PDF for free.
More details 6z3438
- Words: 1,051
- Pages: 12
Forensic Mnemonics *** Metals *** Lead (Pb) *** As All Metals, it has Mixed action: -
Local : G.I.T
Remote : Target Organs can be coded by its chemical symbol:
Pb
Peripheral Nerves
Proximal Tubules of the Kidney blood brain bone A Target organ I always 4get is Kidney, so to :) The main use of Pb when came up was Water pipes.
So, do u the organ with the Largest Water channel system in the Body? Yes, it’s the Kidney, so don’t 4get to mention the Kidney as a target organ in Both Acute & Chronic Lead poisoning, producing (Fanconi – Like syndrome) (Reveraible) ; -Due to Proximal Tubule affection; Glucosuria, Aminoaciduria, Phosphaturia, Albumin, Blood & Casts in Urine. *** Occupational Exposure to Lead can also be coded by its Chemical Symbol:
Pb Plumbers Painters
Petroleum Industry Workers (N.B. Tetra Ethyl Lead (
(exposed to: TEL “Organo lead”)
TEL) is the Most LEThal & rapidly produces Encephalopathy).
battery & bullet (Missile) Industries ***
Special Features of PLumbism
-
LOCal: GIT
Don’t 4get to talk about 3
CO
COLors COLic COnstipation Colors Oral: Blue line at gingival Line (PbS) Intestinal: Black Offensive stool (PbS) Colic:
Paroxysmal & relieved by Pressure. Constipation: With Black offensive stool (PbS) *** Blood & Vascular System
A, B, C
A nemia
(Microcytic Hypochromic), due to:
Haemo-lysis (++ Fragility of RBC’s _ interferes with Na\K Pump & attaches to the membrane >> ++ Fragility)
Heme-Synthesis (inhibition of several Enzymes in Heme Synthesis Pathway through binding to their SH- group)
- With subsequent Compensatory Release of Immature RBC’s (Reticulocytes) Reticulocytosis.
Basophilic stippling
*** (Punctate Basophilia), due to:
Inhibition of Pyridine –5- Nucleotidase (Responsible for Breakdown of RNA)
Clumping of Ribosomal RNA. ***
Circum Oral Pallor, due to VC. *** Peripheral Nerves Lead Palsy (Wrist & Foot Drop)
PlumbuM produces
Purely Motor Peripheral Neuritis, esp. affecting Extensors. *** Proximal Tubules of the Kidney: Fanconi-Like Syndrome.
*** Brain: Encephalopathy. Esp. in Children (Immature BBB) Esp. with TEL. *** Bone: Bone aches & Arthritic pain (Lead esp. deposits near ts) *** Others:
-
Plumbum affects Parents ♀ Abortion (ecboilc) ♂ Sterility & Impotence
-
Plumb
UM affects MyocardiUM (Miocarditis) ***
Regarding Investigations:
-
One of the important investigations in
Lead poisoning, is
detection of
Amino-
Levulinic Acid in urine (++ ALA, due to inhibition of ALA Dehydratase enzyme in Heme synthesis pathway). *** Regarding TTT
PROphylaxis through: PROmote adequate supply of Ca, Zn & Fe. (-- Pb absorption) PROper Ventilation PROtective clothing, Masks, gloves & boots. PERiOdic Medical Examination of exposed workers. *** Regarding the Chelator
B L
( A )
-It’s excreted in
BiLe, so the chelator of choice in Renal Compromise
-It’s contraindicated in
-
Concurrent istration or toxicity of
4F
Fe
Fe-BAL Complex is
toxic.
-
Favism (G6PD Deficiency) Haemolysis. - Liver Failure (excreted in Bile). - Fetal Gestation (Pregnancy). *** Arsenic ***
Acute A
RsEniC ***
As all Metals, mixed action: Local: G.I.T -
Nausea, vomiting, colic, Diarrhea with -
-
RiCE stools
DD : Cholera,
To the points of Differentiation, ask yourself this Qu:
How
To it’s ChOLera or ArSENIc Toxicity ?
Temperature Vomiting COLic ANALYsIs Tenesmus ***
ENic
Remote: Ars
-
Par
ENchymatous organs (Liver, Kidney & Heart) *** Chronic
-Local: G.I.T:
Arsenic:
Anorexia, diarrhea Alternating with Constipation. - Remote: As acute +
Aplastic Anemia Skin & MM.
Peripheral Neuritis; Mainly
Sensory
*** Iron *** Acute Iron Toxicity Condition of Poisoning: Mainly
Accidental, esp. in Children as Iron Preparations are: Attractive, similar to candies. - Available at home. Mechanism of Action: -
-
Local:
GIT: Corrosive effect; may cause Hemorrhagic Necrosis & Perforation.
-
To this Hemorrhagic action, that the Chief Role of Iron in the Body is incorporation in Hemoglobin of RBC’s (Blood cell Synthesis), in contrast, when in excess, it causes (Blood Loss), Hemorrhagic Necrosis. -
-
Remote:
To all Systems affected, these actions coded by
3
P
Peri-portal Blood
Necrosis (Liver)
Pressure (Hypotension) (Cardiovascular)
Blood
PH (Metabolic Acidosis) (Metabolism) ***
To what causes stage I & II in acute Iron Toxicity, Stage I. G -
i
.i . T
Due to rritant Corrosive effect of Iron. *** Stage II. Apparent
-
Due to
Recovery
Redistribution of Iron from Blood to Reticuloendothelial system. ***
N.B. The 2 Main Toxins during our study, targeting the Liver are Iron & Paracetamol; They share some distinct characters: 1- Both are originally handled by liver in Therapeutic doses Iron (Stored in the Liver) Paracetamol (Metabolized in the Liver) 2- When ingested in excess, they Target it, ing Through 4 stages Note that L
IVer
IV 4
The 4 Stages are in order: I. II.
GIT
Apparent Recovery & Altered Blood Chemistry III. Liver Failure & Overt symptoms IV.
Prognosis
See the following Table :) N.B. Pay attention to timing of Stages in each, as a stage may be asked using the time & not the name or symptoms. Iron (Fe) (1-6 hrs) ( 6-24 hrs) ( 12-48 hrs) ( 2-6 Wks) To : F is the
6th
Letter, so 1st stage lasts for
6
hours,
then complete the sequence :)
Paracetamol: (1\2 – 24 hrs) (24-72 hrs) (72-96 hrs) (7-10 days)
Stage
• Stage I •G.I.T
• Stage II •Apparent Recovery (Both) •Altered Blood Chemistry (Paracetamol).
• Stage III
• Liver Failure
Iron
Paracetamol
• Abdominal pain.
• Malaise & Diaphoresis.
• Nausea, Vomiting,
• Nausea & Vomiting.
• Shock & Dehydration from Fluid Loss. • ـــــــــــــــــــ
• Drowsiness (No loss of consciousness) • ـــــــــــــــــــ
Hematemesis & Melena.
• The patient appears falsely stable for a time. • ـــــــــــــــــــ • Hepatic Necrosis & Liver cell failure . • Lethargy & Coma.
• Liver failure
•(But don't 4get that iron in addition has a corrosive effect & targets CVS & Metabolism, so add:
• (Jaundice, Coagulation defects, encephalopathy & Altered concious level)
• Recurrence of G.I.T Symptoms. • Shock, Hypotension & Metabolic acidosis.
• Stage IV • Prognosis
• Pain & Tenderness in Rt. Hypochondrium. • Altered Liver Function Tests. • ـــــــــــــــــــ
• ـــــــــــــــــــ • G.I.T Scarring & Narrowing • with or without Obstruction (Pylorostenosis, Gastric Fibrosis or small bowel stricture).
• ـــــــــــــــــــ • Recovery: Resolution of hepatic dysfunction & complete hepatic recovery within 3 - 6 months. • Death: In severe cases due to Multi-organ failure.
dr R.M
Local : G.I.T
Remote : Target Organs can be coded by its chemical symbol:
Pb
Peripheral Nerves
Proximal Tubules of the Kidney blood brain bone A Target organ I always 4get is Kidney, so to :) The main use of Pb when came up was Water pipes.
So, do u the organ with the Largest Water channel system in the Body? Yes, it’s the Kidney, so don’t 4get to mention the Kidney as a target organ in Both Acute & Chronic Lead poisoning, producing (Fanconi – Like syndrome) (Reveraible) ; -Due to Proximal Tubule affection; Glucosuria, Aminoaciduria, Phosphaturia, Albumin, Blood & Casts in Urine. *** Occupational Exposure to Lead can also be coded by its Chemical Symbol:
Pb Plumbers Painters
Petroleum Industry Workers (N.B. Tetra Ethyl Lead (
(exposed to: TEL “Organo lead”)
TEL) is the Most LEThal & rapidly produces Encephalopathy).
battery & bullet (Missile) Industries ***
Special Features of PLumbism
-
LOCal: GIT
Don’t 4get to talk about 3
CO
COLors COLic COnstipation Colors Oral: Blue line at gingival Line (PbS) Intestinal: Black Offensive stool (PbS) Colic:
Paroxysmal & relieved by Pressure. Constipation: With Black offensive stool (PbS) *** Blood & Vascular System
A, B, C
A nemia
(Microcytic Hypochromic), due to:
Haemo-lysis (++ Fragility of RBC’s _ interferes with Na\K Pump & attaches to the membrane >> ++ Fragility)
Heme-Synthesis (inhibition of several Enzymes in Heme Synthesis Pathway through binding to their SH- group)
- With subsequent Compensatory Release of Immature RBC’s (Reticulocytes) Reticulocytosis.
Basophilic stippling
*** (Punctate Basophilia), due to:
Inhibition of Pyridine –5- Nucleotidase (Responsible for Breakdown of RNA)
Clumping of Ribosomal RNA. ***
Circum Oral Pallor, due to VC. *** Peripheral Nerves Lead Palsy (Wrist & Foot Drop)
PlumbuM produces
Purely Motor Peripheral Neuritis, esp. affecting Extensors. *** Proximal Tubules of the Kidney: Fanconi-Like Syndrome.
*** Brain: Encephalopathy. Esp. in Children (Immature BBB) Esp. with TEL. *** Bone: Bone aches & Arthritic pain (Lead esp. deposits near ts) *** Others:
-
Plumbum affects Parents ♀ Abortion (ecboilc) ♂ Sterility & Impotence
-
Plumb
UM affects MyocardiUM (Miocarditis) ***
Regarding Investigations:
-
One of the important investigations in
Lead poisoning, is
detection of
Amino-
Levulinic Acid in urine (++ ALA, due to inhibition of ALA Dehydratase enzyme in Heme synthesis pathway). *** Regarding TTT
PROphylaxis through: PROmote adequate supply of Ca, Zn & Fe. (-- Pb absorption) PROper Ventilation PROtective clothing, Masks, gloves & boots. PERiOdic Medical Examination of exposed workers. *** Regarding the Chelator
B L
( A )
-It’s excreted in
BiLe, so the chelator of choice in Renal Compromise
-It’s contraindicated in
-
Concurrent istration or toxicity of
4F
Fe
Fe-BAL Complex is
toxic.
-
Favism (G6PD Deficiency) Haemolysis. - Liver Failure (excreted in Bile). - Fetal Gestation (Pregnancy). *** Arsenic ***
Acute A
RsEniC ***
As all Metals, mixed action: Local: G.I.T -
Nausea, vomiting, colic, Diarrhea with -
-
RiCE stools
DD : Cholera,
To the points of Differentiation, ask yourself this Qu:
How
To it’s ChOLera or ArSENIc Toxicity ?
Temperature Vomiting COLic ANALYsIs Tenesmus ***
ENic
Remote: Ars
-
Par
ENchymatous organs (Liver, Kidney & Heart) *** Chronic
-Local: G.I.T:
Arsenic:
Anorexia, diarrhea Alternating with Constipation. - Remote: As acute +
Aplastic Anemia Skin & MM.
Peripheral Neuritis; Mainly
Sensory
*** Iron *** Acute Iron Toxicity Condition of Poisoning: Mainly
Accidental, esp. in Children as Iron Preparations are: Attractive, similar to candies. - Available at home. Mechanism of Action: -
-
Local:
GIT: Corrosive effect; may cause Hemorrhagic Necrosis & Perforation.
-
To this Hemorrhagic action, that the Chief Role of Iron in the Body is incorporation in Hemoglobin of RBC’s (Blood cell Synthesis), in contrast, when in excess, it causes (Blood Loss), Hemorrhagic Necrosis. -
-
Remote:
To all Systems affected, these actions coded by
3
P
Peri-portal Blood
Necrosis (Liver)
Pressure (Hypotension) (Cardiovascular)
Blood
PH (Metabolic Acidosis) (Metabolism) ***
To what causes stage I & II in acute Iron Toxicity, Stage I. G -
i
.i . T
Due to rritant Corrosive effect of Iron. *** Stage II. Apparent
-
Due to
Recovery
Redistribution of Iron from Blood to Reticuloendothelial system. ***
N.B. The 2 Main Toxins during our study, targeting the Liver are Iron & Paracetamol; They share some distinct characters: 1- Both are originally handled by liver in Therapeutic doses Iron (Stored in the Liver) Paracetamol (Metabolized in the Liver) 2- When ingested in excess, they Target it, ing Through 4 stages Note that L
IVer
IV 4
The 4 Stages are in order: I. II.
GIT
Apparent Recovery & Altered Blood Chemistry III. Liver Failure & Overt symptoms IV.
Prognosis
See the following Table :) N.B. Pay attention to timing of Stages in each, as a stage may be asked using the time & not the name or symptoms. Iron (Fe) (1-6 hrs) ( 6-24 hrs) ( 12-48 hrs) ( 2-6 Wks) To : F is the
6th
Letter, so 1st stage lasts for
6
hours,
then complete the sequence :)
Paracetamol: (1\2 – 24 hrs) (24-72 hrs) (72-96 hrs) (7-10 days)
Stage
• Stage I •G.I.T
• Stage II •Apparent Recovery (Both) •Altered Blood Chemistry (Paracetamol).
• Stage III
• Liver Failure
Iron
Paracetamol
• Abdominal pain.
• Malaise & Diaphoresis.
• Nausea, Vomiting,
• Nausea & Vomiting.
• Shock & Dehydration from Fluid Loss. • ـــــــــــــــــــ
• Drowsiness (No loss of consciousness) • ـــــــــــــــــــ
Hematemesis & Melena.
• The patient appears falsely stable for a time. • ـــــــــــــــــــ • Hepatic Necrosis & Liver cell failure . • Lethargy & Coma.
• Liver failure
•(But don't 4get that iron in addition has a corrosive effect & targets CVS & Metabolism, so add:
• (Jaundice, Coagulation defects, encephalopathy & Altered concious level)
• Recurrence of G.I.T Symptoms. • Shock, Hypotension & Metabolic acidosis.
• Stage IV • Prognosis
• Pain & Tenderness in Rt. Hypochondrium. • Altered Liver Function Tests. • ـــــــــــــــــــ
• ـــــــــــــــــــ • G.I.T Scarring & Narrowing • with or without Obstruction (Pylorostenosis, Gastric Fibrosis or small bowel stricture).
• ـــــــــــــــــــ • Recovery: Resolution of hepatic dysfunction & complete hepatic recovery within 3 - 6 months. • Death: In severe cases due to Multi-organ failure.
dr R.M
Related Documents c2h70

Forensic Mnemonics - Metals 4h1de
January 2022 0
Mnemonics Forensic Medicine 5y5cq
October 2019 80
Forensic 69222v
November 2019 97
Mnemonics 5q3n4x
December 2021 0
Mnemonics 5q3n4x
December 2020 0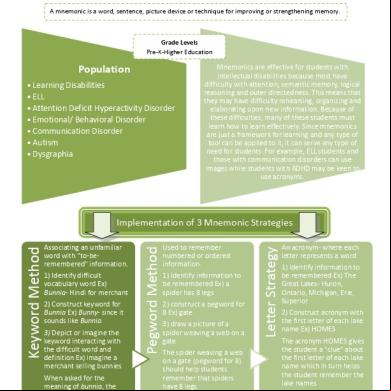
Mnemonics 5q3n4x
December 2019 137More Documents from "Riham Mohye Eldeen Mohammed" 6i5v68
Forensic Mnemonics - Metals 4h1de
January 2022 0
Ent Mnemonics 1 74m4c
October 2019 129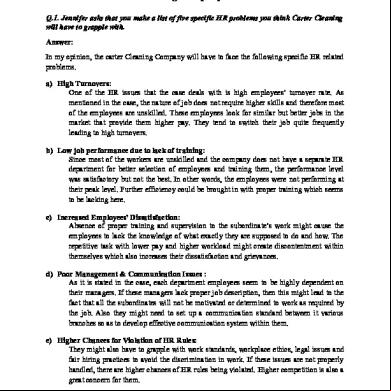
Solution-to-carter-cleaning-company.docx 23m1r
December 2021 0
Essential Grammar Of German - With Exercises - Mit 40 Abbildungen.1-vorschau 6f1y41
December 2019 44
6g3p1u
December 2021 0