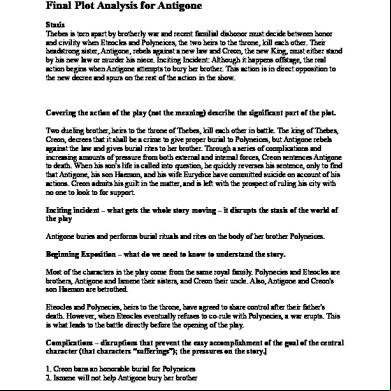
Case Study (peptic Ulcer) 4m325o
This document was ed by and they confirmed that they have the permission to share it. If you are author or own the copyright of this book, please report to us by using this report form. Report 2z6p3t
Overview 5o1f4z
& View Case Study (peptic Ulcer) as PDF for free.
More details 6z3438
- Words: 965
- Pages: 26
GROUP 7 Pamintuan, Adie Kim Quetua, sca Marie Robles, Ma. Cecilia Santos, Amalia Tapaoan, Symphony Jane
CASE 1 (FINALS)
CHIEF COMPLAINT “My stomach has been hurting for the past weeks. Over the weekend I noticed my bowel movements were black and tarry.”
PATIENT DEMOGRAPHICS William Smith Male 62 years old Height: 5’9’’ Weight: 102kg
HISTORY OF PRESENT ILLNESS Intermittent burning epigastric pain for more than 2 months. Intermittent belching, bloated, weak when walking and nausea after eating. Pain in right epigastrium, worse with meals.
HISTORY OF PRESENT ILLNESS Black, tarry bowel movements No PUD or GI bleeding No anorexia or vomiting
PAST MEDICAL HISTORY COPD (Chronic Obstructive Pulmonary Disease) x 10 years DM (Diabetes Mellitus) x 10 years Osteoarthritis x 15 years (right shoulder)
FAMILY HISTORY
Father died at 55: Acute Myocardial Infarction (MI) Mother died at 65: Lung Cancer (CA) 3 siblings alive and well
SOCIAL HISTORY ant Married and has 3 daughters Smokes cigar occasionally Drinks beer per week
REVIEW OF SYSTEMS Unremarkable except for complaints noted above
ALLERGY: Penicillins – hives PHYSICAL EXAMINATION: General Overweight man in moderate distress SKIN: Warm and dry HEENT: PERRLA, EOMI, discs flat, no AV nicking, hemorrhages, or exudates CHEST: Bilateral rhonchi, faint wheezes
REVIEW OF SYSTEMS CARDIOVASCULAR: S1, S2 normal; no MRG ABDOMEN: Normal bowel sounds and mild epigastric tenderness; liver size normal; no splenomegaly or masses observed RECTAL: Nontender,; melenic stool found in rectal vault; stool heme (+) EXTENSION: Normal ROM except for restricted right shoulder movement NEURO: CN II-XII intact, DTRs 2 + throughout
VITAL SIGNS BLOOD PRESSURE: 120/62 PULSE: 109 RESPIRATORY RATE:18 TEMPERATURE:37.9
LABORATORY RESULTS RESULTS SODIUM 144 meq/l HEMOGLOBIN 9.2 g/dl CALCIUM 9.2 mg/dl POTASSIUM 3.9 meq/l HEMATOCRIT 26.2% MAGNESIUM 2.0 meq/l
REMARKS X √ X X √ √
LABORATORY RESULTS RESULTS CHLORIDE 98 meq/l IRON 49 mcg/dl PHOSPHORUS 4.0mg/dl CARBON DIOXIDE
REMARKS X √ X √
LABORATORY RESULTS RESULTS
REMARKS
ALBUMIN 3.9 g/dL
X
BLOOD UREA NITROGEN 10 mg/dL
X
FASTING BLOOD GLUCOSE 154 mg/dL
√
MEAN CORPUSCULAR VOL 74 mm3
√
PLATELET 230 X 103 /mm3 RETICULOCYTES 0.3% SERUM CREATININE 1.1 mg/dL WHITE BLOOD CELLS 8.4 x 103/mm3
X √ X X
DIAGNOSTIC PROCEDURES Endoscopy 6-mm ulcer in the gastric antrum Peripheral Blood Smear (+) for Microcytic anemia
ABBREVIATIONS PUD – Peptic Ulcer Disease GI – Gastrointestinal PERRLA -Pupils Equal, Round, Reactive to Light and Accommodation EOMI –Extra ocular Movements Intact AV – Atriovenous ROM – Range of Motion CN – Cranial Nerve DTR – Deep Tendon Reflex
MEDICATIONS DRUGS METFORMIN (Glucophage®)
MOA
INDICATION
Reduce hepatic glucose through activation of AMPK
Type II Diabetes
Lactic acidosis, CHF, hypoxic/acidotic states
Irreversible inactivation of the cyclooxygenase (COX) enzyme
Reduce fever and relieve mild to moderate pain from conditions such as muscle aches
Stomach upset, heartburn
Short acting muscarinic antagonist
Long-term treatment of reversible bronchospasm associated with COPD
urinary tract infection, upper respiratory tract infection, sinusitis, bronchitis, and exacerbation of COPD
500mg PO BID ASA (Aspirin EC®) 325mg PO once daily IPRATROPIUM MDI (Atrovent®) 2 puffs 4x daily
ADR
MEDICATIONS DRUG ALBUTEROL MDI (Ventolin®) 2 puffs PRN IBUPROFEN (Advil®)
MOA
INDICATION
Short-acting, selective B2adrenergic receptor agonist
Asthma and COPD
Acute infection of the nose, throat, sinus, fast heartbeat, feeling of throwing up
Related to (NSAIDs), prostaglandin synthetase inhibition
Used to reduce fever and treat pain or inflammation
Hemorrhage, vomiting, hypertension, eosinophilia, and anemia
Neutralizes gastric pH
Heartburn, acid indigestion, sour stomach, upset stomach
Nausea, constipation, diarrhea, headache
200mg 2 tabs PRN Mg Hydroxide, Al Hydroxide (Maalox®) 1 tbsp. PRN
ADR
DRUG INTERACTION Alcohol & metformin -causes Lactic acidosis Ibuprofen & Aspirin - increase your risk of developing gastrointestinal ulcers and bleeding - may cause severe abdominal pain, bloating, loss of appetite, and/or black, tarry stools Albuterol & Magnesium Hydroxide (MAALOX) - irregular heart rhythm that may be serious and potentially life-threatening: risk is increased if you have low blood levels of magnesium or potassium
ASSESMENT PHYSIOLOGY STOMACH
Breaks down large food particles into smaller pieces so that they can be processed more easily. It is intraperitonal and located in the left epigastric regions of the abdomen.
Hydrochloric acid -secreted from the parietal cells in the body of the stomach.
PATHOPHYSIOLOGY
Peptic ulcer - is a circumscribed loss of the mucus membrane of the GIT system exposed to gastric juices containing acid & pepsin. Peptic ulcer occur most common in: -esophagus -stomach*
Imbalance Of This Factors Causes Peptic Ulcer Disease: Aggressive factors -bile, acid and pepsin Defensive factors -mucus, bicarbonates and PG
Other contributory factors:
Helicobacter pylori NSAIDs Stress Ethanol Tobacco
Complications of PUD 1. Bleeding - occurs in 25-30% of patients -most frequent complication and maybe life threatening - for 25% of ulcers deaths 2. Perforation -occurs in about 5% of the patients -s for 2/3 of ulcer deaths 3. Obstruction from edema or scarring
PHARMACOTHERAPHY Misoprostol -may be used to prevent gastric ulcers caused by non-steroidal anti- inflammatory drugs.
Consider that the interaction may be unavoidable if ibuprofen is istered more than once daily. Avoid ibuprofen if possible or give it 2 hours after aspirin. Consider alternative: Acetaminophen* reduces pain and lowers fevers. Unlike aspirin and other NSAIDS, acetaminophen is believed to be safe for people with ulcers.
NON-PHARMACOTHERAPY Refer the patient to a smoking-cessation program Stress Reduction Avoidance of dietary irritants (Alcohol) Physical activity can help reduce some kinds of discomfort, such as arthritis pain.
REFERENCES -MEDSCAPE -WEBMD -DRUGS.COM -MEDLINEPLUS MEDICAL ENCYLOPEDIA -Katzung et.al., Basic and Clinical Pharmacology (p. 355 &757)
CASE 1 (FINALS)
CHIEF COMPLAINT “My stomach has been hurting for the past weeks. Over the weekend I noticed my bowel movements were black and tarry.”
PATIENT DEMOGRAPHICS William Smith Male 62 years old Height: 5’9’’ Weight: 102kg
HISTORY OF PRESENT ILLNESS Intermittent burning epigastric pain for more than 2 months. Intermittent belching, bloated, weak when walking and nausea after eating. Pain in right epigastrium, worse with meals.
HISTORY OF PRESENT ILLNESS Black, tarry bowel movements No PUD or GI bleeding No anorexia or vomiting
PAST MEDICAL HISTORY COPD (Chronic Obstructive Pulmonary Disease) x 10 years DM (Diabetes Mellitus) x 10 years Osteoarthritis x 15 years (right shoulder)
FAMILY HISTORY
Father died at 55: Acute Myocardial Infarction (MI) Mother died at 65: Lung Cancer (CA) 3 siblings alive and well
SOCIAL HISTORY ant Married and has 3 daughters Smokes cigar occasionally Drinks beer per week
REVIEW OF SYSTEMS Unremarkable except for complaints noted above
ALLERGY: Penicillins – hives PHYSICAL EXAMINATION: General Overweight man in moderate distress SKIN: Warm and dry HEENT: PERRLA, EOMI, discs flat, no AV nicking, hemorrhages, or exudates CHEST: Bilateral rhonchi, faint wheezes
REVIEW OF SYSTEMS CARDIOVASCULAR: S1, S2 normal; no MRG ABDOMEN: Normal bowel sounds and mild epigastric tenderness; liver size normal; no splenomegaly or masses observed RECTAL: Nontender,; melenic stool found in rectal vault; stool heme (+) EXTENSION: Normal ROM except for restricted right shoulder movement NEURO: CN II-XII intact, DTRs 2 + throughout
VITAL SIGNS BLOOD PRESSURE: 120/62 PULSE: 109 RESPIRATORY RATE:18 TEMPERATURE:37.9
LABORATORY RESULTS RESULTS SODIUM 144 meq/l HEMOGLOBIN 9.2 g/dl CALCIUM 9.2 mg/dl POTASSIUM 3.9 meq/l HEMATOCRIT 26.2% MAGNESIUM 2.0 meq/l
REMARKS X √ X X √ √
LABORATORY RESULTS RESULTS CHLORIDE 98 meq/l IRON 49 mcg/dl PHOSPHORUS 4.0mg/dl CARBON DIOXIDE
REMARKS X √ X √
LABORATORY RESULTS RESULTS
REMARKS
ALBUMIN 3.9 g/dL
X
BLOOD UREA NITROGEN 10 mg/dL
X
FASTING BLOOD GLUCOSE 154 mg/dL
√
MEAN CORPUSCULAR VOL 74 mm3
√
PLATELET 230 X 103 /mm3 RETICULOCYTES 0.3% SERUM CREATININE 1.1 mg/dL WHITE BLOOD CELLS 8.4 x 103/mm3
X √ X X
DIAGNOSTIC PROCEDURES Endoscopy 6-mm ulcer in the gastric antrum Peripheral Blood Smear (+) for Microcytic anemia
ABBREVIATIONS PUD – Peptic Ulcer Disease GI – Gastrointestinal PERRLA -Pupils Equal, Round, Reactive to Light and Accommodation EOMI –Extra ocular Movements Intact AV – Atriovenous ROM – Range of Motion CN – Cranial Nerve DTR – Deep Tendon Reflex
MEDICATIONS DRUGS METFORMIN (Glucophage®)
MOA
INDICATION
Reduce hepatic glucose through activation of AMPK
Type II Diabetes
Lactic acidosis, CHF, hypoxic/acidotic states
Irreversible inactivation of the cyclooxygenase (COX) enzyme
Reduce fever and relieve mild to moderate pain from conditions such as muscle aches
Stomach upset, heartburn
Short acting muscarinic antagonist
Long-term treatment of reversible bronchospasm associated with COPD
urinary tract infection, upper respiratory tract infection, sinusitis, bronchitis, and exacerbation of COPD
500mg PO BID ASA (Aspirin EC®) 325mg PO once daily IPRATROPIUM MDI (Atrovent®) 2 puffs 4x daily
ADR
MEDICATIONS DRUG ALBUTEROL MDI (Ventolin®) 2 puffs PRN IBUPROFEN (Advil®)
MOA
INDICATION
Short-acting, selective B2adrenergic receptor agonist
Asthma and COPD
Acute infection of the nose, throat, sinus, fast heartbeat, feeling of throwing up
Related to (NSAIDs), prostaglandin synthetase inhibition
Used to reduce fever and treat pain or inflammation
Hemorrhage, vomiting, hypertension, eosinophilia, and anemia
Neutralizes gastric pH
Heartburn, acid indigestion, sour stomach, upset stomach
Nausea, constipation, diarrhea, headache
200mg 2 tabs PRN Mg Hydroxide, Al Hydroxide (Maalox®) 1 tbsp. PRN
ADR
DRUG INTERACTION Alcohol & metformin -causes Lactic acidosis Ibuprofen & Aspirin - increase your risk of developing gastrointestinal ulcers and bleeding - may cause severe abdominal pain, bloating, loss of appetite, and/or black, tarry stools Albuterol & Magnesium Hydroxide (MAALOX) - irregular heart rhythm that may be serious and potentially life-threatening: risk is increased if you have low blood levels of magnesium or potassium
ASSESMENT PHYSIOLOGY STOMACH
Breaks down large food particles into smaller pieces so that they can be processed more easily. It is intraperitonal and located in the left epigastric regions of the abdomen.
Hydrochloric acid -secreted from the parietal cells in the body of the stomach.
PATHOPHYSIOLOGY
Peptic ulcer - is a circumscribed loss of the mucus membrane of the GIT system exposed to gastric juices containing acid & pepsin. Peptic ulcer occur most common in: -esophagus -stomach*
Imbalance Of This Factors Causes Peptic Ulcer Disease: Aggressive factors -bile, acid and pepsin Defensive factors -mucus, bicarbonates and PG
Other contributory factors:
Helicobacter pylori NSAIDs Stress Ethanol Tobacco
Complications of PUD 1. Bleeding - occurs in 25-30% of patients -most frequent complication and maybe life threatening - for 25% of ulcers deaths 2. Perforation -occurs in about 5% of the patients -s for 2/3 of ulcer deaths 3. Obstruction from edema or scarring
PHARMACOTHERAPHY Misoprostol -may be used to prevent gastric ulcers caused by non-steroidal anti- inflammatory drugs.
Consider that the interaction may be unavoidable if ibuprofen is istered more than once daily. Avoid ibuprofen if possible or give it 2 hours after aspirin. Consider alternative: Acetaminophen* reduces pain and lowers fevers. Unlike aspirin and other NSAIDS, acetaminophen is believed to be safe for people with ulcers.
NON-PHARMACOTHERAPY Refer the patient to a smoking-cessation program Stress Reduction Avoidance of dietary irritants (Alcohol) Physical activity can help reduce some kinds of discomfort, such as arthritis pain.
REFERENCES -MEDSCAPE -WEBMD -DRUGS.COM -MEDLINEPLUS MEDICAL ENCYLOPEDIA -Katzung et.al., Basic and Clinical Pharmacology (p. 355 &757)
Related Documents c2h70

Case Study (peptic Ulcer) 4m325o
May 2020 25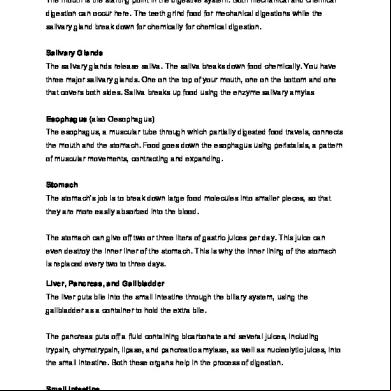
Bleeding Peptic Ulcer Disease Case Study 76d63
February 2022 0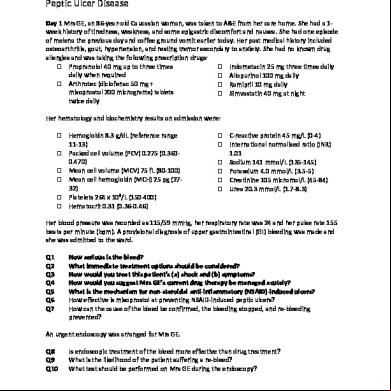
Case Study Peptic Ulcer Disease-1.docx 46523s
December 2021 0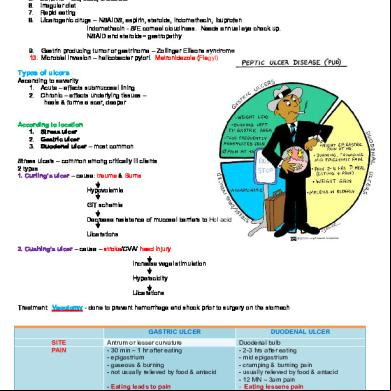
Peptic Ulcer 5x7272
November 2020 0
Case Presentation On Peptic Ulcer 2z3eo
November 2019 103
Peptic Ulcer Disease 4531w
December 2019 35More Documents from "Precious" 2i4z5a
Case Study (peptic Ulcer) 4m325o
May 2020 25
An Outlook On Ariel S. Tabag's Voice Tape q4i
December 2019 166
[jonathan Glover] Causing Death And Saving Lives(bookfi.org) Copy 1m4h3c
November 2019 41
Gospel Songs 383c3i
November 2021 0
Living-in-christ - Billy Graham.pdf 4i395a
October 2019 109