Annual Medical Report Form 4mq6s
This document was ed by and they confirmed that they have the permission to share it. If you are author or own the copyright of this book, please report to us by using this report form. Report 2z6p3t
Overview 5o1f4z
& View Annual Medical Report Form as PDF for free.
More details 6z3438
- Words: 1,267
- Pages: 8
Republic of the Philippines Department of Labor and Employment National Capital Region
ANNUAL MEDICAL REPORT FORM For Period January 1, _____ to December 31, _____
1. Name of Establishment:__________________________________________________ 2. Address:______________________________________________________________ 3. Name of Owner/ Manager:________________________________________________ 4. Nature of Business & Product/ Service (Ex. Manufacturing – textile)_______________ ________________________________________________________________________ 5. Total Number of Employee:_________ Number of Shift:________________________ 6. Number Distribution of Employee as to nature/workplace, sex & workship: office Male :___________ Female:__________ Total:___________
1st Shift ___________ ___________ ___________
Product/Shop 2nd Shift ______________ ______________ ______________
3rd Shift ____________ ____________ ____________
7. Preventive Occupational Health Service: (Check or Cross) a. Occupational health service is organized / provided by: ( ) the establishment / undertaking ( ) government authority / institution ( ) other bodies / group / institution ( specify )__________________________ ____________________________________________________________ b. Occupational health services as described under number 7a above, is organized / provided as a service : ( ) solely for the workers of the establishment / undertakings ( ) common to a number of establishment / undertakings
1
c. The employer engages the services of : ( ) Occupational health practitioner Name: ______________________________________________________ Address: ____________________________________________________ ( ) Occupational health physician Name: ______________________________________________________ Address: ____________________________________________________ ( ) Occupational health dentist Name: ______________________________________________________ Address: ____________________________________________________ ( ) Occupational health nurse Name: ______________________________________________________ Address: ____________________________________________________ d. The occupational health physician/practitioner/nurse/personnel conducts an inspection of the work place: ( ) once every month ( ) once every two (2) months ( ) once every three (3) months ( ) once every six (6) months ( ) other details: _________________________________________________ __________________________________________________ 8. Emergency Occupational Health Services: a. The employer provides a treatment room/medical clinic in the work place with medicines and facilities ( ) Yes _________________ ( ) No __________________ ( ) others, please specify __________________________________________ ____________________________________________________________ b. Schedule of attendance in the work place: Occupational health physician Occupational health dentist
:________ :________
c. Schedule of attendance of full time first aider ( ) 1st work shift ( )2nd work shift ( ) 3rd work shift
2
Work shift hrs./day___________ hrs/day ___________
d. The following occupational health personal of this establishment have under gone training in occupation health and safety/first aid : ( ) Occupational health physician ( ) Occupation health dentist ( ) Occupation health nurse ( ) first - aider ( ) Others, please specify___________________________________________ ____________________________________________________________ 9. Occupational Health Services a. The occupational health personnel of this establishment regular appraisal of the sanitation system in the workplace: ( ) Yes
( ) No
b. Number of workers who underwent the following medical examinations:
1. 2. 3. 4. 5. 6.
1. 2. 3. 4. 5. 6.
Pre-placement Periodic Return-to –work Transfer Special Separation
Physical Exam ____________ ____________ ____________ ____________ ____________ ____________
Pre-placement Periodic Return-to-work Transfer Special Separation
Stool Exam ______ ______ ______ ______ ______ ______
-3-
X-rays ________ ________ ________ ________ ________ ________
Blood Test ______ ______ ______ ______ ______ ______
Urinalysis ___________ ____________ ____________ ____________ ____________ ____________
ECG
Others
______ ______ ______ ______ ______ ______
______ ______ ______ ______ ______ ______
10. Report of Diseases a. Number of consultations/treatments for the following diseases: Male
Female
Total No. Of Cases
______ ______
_______ _______
__________ __________
______ ______
_______ _______
__________ __________
______ ______
_______ _______
__________ __________
______
_______
__________
______ ______ ______
_______ _______ _______
__________ __________ __________
______
_______
__________
______
_______
__________
______ ______
_______ _______
__________ __________
______ ______ ______ ______
_______ _______ _______ _______
__________ __________ __________ __________
Skin: ( ) Allergy ( ) Dermatoses ( ) Infection as folliculitis abscess/paronychia ( ) Others Head: ( ) Tension/headache ( ) Others Eyes: ( ) Error of refraction ( ) Bacterial/Viral conjunctivities ( ) Cataract ( ) Others Mouth & ENT: ( ) Gingivitis ( ) Herpes Labiales/ nasalis ( ) Otitis Media Externa ( ) Deafness ( ) Meniere”s Syndrome /Vertigo ( ) Rhinitis/Colds ( ) Nasal Polyps ( ) Sinusitis ( ) Tonsilio
4
pharyngitis ( ) Laryngitis ( ) Others
______ ______ ______
_______ _______ _______
__________ __________ __________
Respiratory: ( ( ( ( ( (
) ) ) ) ) )
Bronchitis Bronchial/Asthma Pneumonia Tuberculosis Pneumoconiosis Others
______ ______ ______ ______ ______ ______
_______ _______ _______ _______ _______ _______
__________ __________ __________ __________ __________ __________
______ ______ ______
_______ _______ _______
__________ __________ __________
______
_______
__________
______ ______
_______ _______
__________ __________
______ ______
_______ _______
__________ __________
______ ______
_______ _______
__________ __________
______
_______
__________
Heart and Blood Vessel: ( ( ( (
) ) ) )
Hypertension Hypotension Angina Pectoris Myocardial Infraction ( ) Vascular disturbances in extremities due to continuous vibration ( ) Others
Gastrointestinal: ( ) Casroenteritis/ Diarrhea ( ) Amoebiasis ( ) Gastritis/ Hyperacidity ( ) Appendicitis ( ) Infectious Hepatitis
5
( ) Liver Cirrhosis ( ) Hepatic Abscess ( ) Cancer (Hepatic/ Gastric) ( ) Ulcer ( ) Others
______ ______
_______ _______
__________ __________
______ ______ ______
_______ _______ _______
__________ __________ __________
______ ______ _____ _____
_______ _______ _______ _______
__________ __________ __________ __________
_____
_______
__________
_____
_______
__________
_____ _____
_______ _______
__________ __________
_____ _____
_______ _______
__________ __________
______
_______
_________
Male
Female
______ ______ ______ ______ ______ ______
________ ________ ________ ________ ________ ________
Total No. Of Cases ___________ ___________ ___________ ___________ ___________ ___________
Genito Urinary: ( ) Urinary Tract infection ( ) Stones ( ) Cancer ( ) Others Reproductive: ( ) Dysmenorrhea ( ) Isfection (Cervicitive) (Vaginitis) ( ) Abortion (Spontaneus) (threatened) ( ) Hyperremesis Gravidarum ( ) Uterine Tumors ( ) Cervical Polyp/ Cancer
12. Immunization Program (Indicate number immunized) Nature Tetanus Toxoid Injection Tetanus Antioxin Injection Tetanus Globulin Injection Hepatitis B Vaccine Rabies Vaccine Others (Please Specify)
6
13. Keeping of Medical Records of Workers (Please Check) ( )
Done
( )
Not Done
14. Health Education and Counseling by Health and Safety Personnel: (Please Check one or more) ( ) ( ) ( )
done individual as each worker comes to the clinic for consultation. done in organized group discussions/seminars. done with the use of visual displays and/or promotional materials, leaflets, etc.
15. Other Health Programs (Please Check) Kinds of Program
Seminars
Nutrition Program Material and Child Care Program Family Planning Program Mental Health Activities Personal Health Maintenance
( ( ( ( (
) ) ) ) )
Use of Visual id/Materials ( ) ( ) ( ) ( ) ( )
Counseling ( ( ( ( (
) ) ) ) )
Physical Fitness Program: (Please Check) Sport Activities Others (Please Check)
( ) Yes ( ) Yes
( ) No ( ) No
16. Hazard in the workplace : (Please check and give details of the substance) Substance and/or sources a. Chemical Hazard: b. ( ) Dust (Ex. Silica dust) ( ) Liquid (Ex. Mercury) ( ) Mist/fumes/vapors (Ex. mist from paint spraying) ( ) Gas (Ex. CO, H2S) ( ) Others (please specify) (Ex. solvents)
Number of workers exposed
_____________ _____________
________________ ________________
_____________ _____________
________________ ________________
_____________
________________
7
Physical Hazards ( ( ( ( ( ( (
) ) ) ) ) ) )
Noise Temperature/humidity Pressure Illumination Radiation/ultraviolet/microwave Vibration Others (Please specify)
c. Biological hazard: ( ( ( ( (
) Viral ) Bacterial ) Fungal ) Parasitic ) Others, specify
_____________ _____________ _____________ _____________ _____________
_________________ _________________ _________________ _________________ _________________
_____________ _____________ _____________ _____________ _____________ _____________
_________________ __________________ __________________ __________________ __________________ __________________
d. Ergonomic Stress: ( ( ( ( ( (
) ) ) ) ) )
Exhausting physical work Prolonged standing Low back pain Unfavorable work posture Static/monotonous work Others, specify
Submitted by: __________________________ Medical Personnel/Title
__________________ Date
Noted by: _______________________________ Employer
ANNUAL MEDICAL REPORT FORM For Period January 1, _____ to December 31, _____
1. Name of Establishment:__________________________________________________ 2. Address:______________________________________________________________ 3. Name of Owner/ Manager:________________________________________________ 4. Nature of Business & Product/ Service (Ex. Manufacturing – textile)_______________ ________________________________________________________________________ 5. Total Number of Employee:_________ Number of Shift:________________________ 6. Number Distribution of Employee as to nature/workplace, sex & workship: office Male :___________ Female:__________ Total:___________
1st Shift ___________ ___________ ___________
Product/Shop 2nd Shift ______________ ______________ ______________
3rd Shift ____________ ____________ ____________
7. Preventive Occupational Health Service: (Check or Cross) a. Occupational health service is organized / provided by: ( ) the establishment / undertaking ( ) government authority / institution ( ) other bodies / group / institution ( specify )__________________________ ____________________________________________________________ b. Occupational health services as described under number 7a above, is organized / provided as a service : ( ) solely for the workers of the establishment / undertakings ( ) common to a number of establishment / undertakings
1
c. The employer engages the services of : ( ) Occupational health practitioner Name: ______________________________________________________ Address: ____________________________________________________ ( ) Occupational health physician Name: ______________________________________________________ Address: ____________________________________________________ ( ) Occupational health dentist Name: ______________________________________________________ Address: ____________________________________________________ ( ) Occupational health nurse Name: ______________________________________________________ Address: ____________________________________________________ d. The occupational health physician/practitioner/nurse/personnel conducts an inspection of the work place: ( ) once every month ( ) once every two (2) months ( ) once every three (3) months ( ) once every six (6) months ( ) other details: _________________________________________________ __________________________________________________ 8. Emergency Occupational Health Services: a. The employer provides a treatment room/medical clinic in the work place with medicines and facilities ( ) Yes _________________ ( ) No __________________ ( ) others, please specify __________________________________________ ____________________________________________________________ b. Schedule of attendance in the work place: Occupational health physician Occupational health dentist
:________ :________
c. Schedule of attendance of full time first aider ( ) 1st work shift ( )2nd work shift ( ) 3rd work shift
2
Work shift hrs./day___________ hrs/day ___________
d. The following occupational health personal of this establishment have under gone training in occupation health and safety/first aid : ( ) Occupational health physician ( ) Occupation health dentist ( ) Occupation health nurse ( ) first - aider ( ) Others, please specify___________________________________________ ____________________________________________________________ 9. Occupational Health Services a. The occupational health personnel of this establishment regular appraisal of the sanitation system in the workplace: ( ) Yes
( ) No
b. Number of workers who underwent the following medical examinations:
1. 2. 3. 4. 5. 6.
1. 2. 3. 4. 5. 6.
Pre-placement Periodic Return-to –work Transfer Special Separation
Physical Exam ____________ ____________ ____________ ____________ ____________ ____________
Pre-placement Periodic Return-to-work Transfer Special Separation
Stool Exam ______ ______ ______ ______ ______ ______
-3-
X-rays ________ ________ ________ ________ ________ ________
Blood Test ______ ______ ______ ______ ______ ______
Urinalysis ___________ ____________ ____________ ____________ ____________ ____________
ECG
Others
______ ______ ______ ______ ______ ______
______ ______ ______ ______ ______ ______
10. Report of Diseases a. Number of consultations/treatments for the following diseases: Male
Female
Total No. Of Cases
______ ______
_______ _______
__________ __________
______ ______
_______ _______
__________ __________
______ ______
_______ _______
__________ __________
______
_______
__________
______ ______ ______
_______ _______ _______
__________ __________ __________
______
_______
__________
______
_______
__________
______ ______
_______ _______
__________ __________
______ ______ ______ ______
_______ _______ _______ _______
__________ __________ __________ __________
Skin: ( ) Allergy ( ) Dermatoses ( ) Infection as folliculitis abscess/paronychia ( ) Others Head: ( ) Tension/headache ( ) Others Eyes: ( ) Error of refraction ( ) Bacterial/Viral conjunctivities ( ) Cataract ( ) Others Mouth & ENT: ( ) Gingivitis ( ) Herpes Labiales/ nasalis ( ) Otitis Media Externa ( ) Deafness ( ) Meniere”s Syndrome /Vertigo ( ) Rhinitis/Colds ( ) Nasal Polyps ( ) Sinusitis ( ) Tonsilio
4
pharyngitis ( ) Laryngitis ( ) Others
______ ______ ______
_______ _______ _______
__________ __________ __________
Respiratory: ( ( ( ( ( (
) ) ) ) ) )
Bronchitis Bronchial/Asthma Pneumonia Tuberculosis Pneumoconiosis Others
______ ______ ______ ______ ______ ______
_______ _______ _______ _______ _______ _______
__________ __________ __________ __________ __________ __________
______ ______ ______
_______ _______ _______
__________ __________ __________
______
_______
__________
______ ______
_______ _______
__________ __________
______ ______
_______ _______
__________ __________
______ ______
_______ _______
__________ __________
______
_______
__________
Heart and Blood Vessel: ( ( ( (
) ) ) )
Hypertension Hypotension Angina Pectoris Myocardial Infraction ( ) Vascular disturbances in extremities due to continuous vibration ( ) Others
Gastrointestinal: ( ) Casroenteritis/ Diarrhea ( ) Amoebiasis ( ) Gastritis/ Hyperacidity ( ) Appendicitis ( ) Infectious Hepatitis
5
( ) Liver Cirrhosis ( ) Hepatic Abscess ( ) Cancer (Hepatic/ Gastric) ( ) Ulcer ( ) Others
______ ______
_______ _______
__________ __________
______ ______ ______
_______ _______ _______
__________ __________ __________
______ ______ _____ _____
_______ _______ _______ _______
__________ __________ __________ __________
_____
_______
__________
_____
_______
__________
_____ _____
_______ _______
__________ __________
_____ _____
_______ _______
__________ __________
______
_______
_________
Male
Female
______ ______ ______ ______ ______ ______
________ ________ ________ ________ ________ ________
Total No. Of Cases ___________ ___________ ___________ ___________ ___________ ___________
Genito Urinary: ( ) Urinary Tract infection ( ) Stones ( ) Cancer ( ) Others Reproductive: ( ) Dysmenorrhea ( ) Isfection (Cervicitive) (Vaginitis) ( ) Abortion (Spontaneus) (threatened) ( ) Hyperremesis Gravidarum ( ) Uterine Tumors ( ) Cervical Polyp/ Cancer
12. Immunization Program (Indicate number immunized) Nature Tetanus Toxoid Injection Tetanus Antioxin Injection Tetanus Globulin Injection Hepatitis B Vaccine Rabies Vaccine Others (Please Specify)
6
13. Keeping of Medical Records of Workers (Please Check) ( )
Done
( )
Not Done
14. Health Education and Counseling by Health and Safety Personnel: (Please Check one or more) ( ) ( ) ( )
done individual as each worker comes to the clinic for consultation. done in organized group discussions/seminars. done with the use of visual displays and/or promotional materials, leaflets, etc.
15. Other Health Programs (Please Check) Kinds of Program
Seminars
Nutrition Program Material and Child Care Program Family Planning Program Mental Health Activities Personal Health Maintenance
( ( ( ( (
) ) ) ) )
Use of Visual id/Materials ( ) ( ) ( ) ( ) ( )
Counseling ( ( ( ( (
) ) ) ) )
Physical Fitness Program: (Please Check) Sport Activities Others (Please Check)
( ) Yes ( ) Yes
( ) No ( ) No
16. Hazard in the workplace : (Please check and give details of the substance) Substance and/or sources a. Chemical Hazard: b. ( ) Dust (Ex. Silica dust) ( ) Liquid (Ex. Mercury) ( ) Mist/fumes/vapors (Ex. mist from paint spraying) ( ) Gas (Ex. CO, H2S) ( ) Others (please specify) (Ex. solvents)
Number of workers exposed
_____________ _____________
________________ ________________
_____________ _____________
________________ ________________
_____________
________________
7
Physical Hazards ( ( ( ( ( ( (
) ) ) ) ) ) )
Noise Temperature/humidity Pressure Illumination Radiation/ultraviolet/microwave Vibration Others (Please specify)
c. Biological hazard: ( ( ( ( (
) Viral ) Bacterial ) Fungal ) Parasitic ) Others, specify
_____________ _____________ _____________ _____________ _____________
_________________ _________________ _________________ _________________ _________________
_____________ _____________ _____________ _____________ _____________ _____________
_________________ __________________ __________________ __________________ __________________ __________________
d. Ergonomic Stress: ( ( ( ( ( (
) ) ) ) ) )
Exhausting physical work Prolonged standing Low back pain Unfavorable work posture Static/monotonous work Others, specify
Submitted by: __________________________ Medical Personnel/Title
__________________ Date
Noted by: _______________________________ Employer
Related Documents c2h70

Annual Medical Report Form 4mq6s
December 2019 81
11 - Annual Medical Report Form 6tp2q
October 2022 0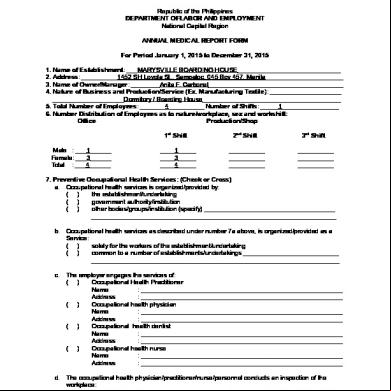
Annual Medical Report 4m461d
November 2019 44
Annual Confidential Report Form 6q6j2j
October 2019 34
Annual Medical Report Form (dole_bwc_hsd_)h-47-a) 5l6h3w
December 2019 55
Medical Form 3e62w
November 2019 83More Documents from "Nellie Ramos" 5q1h6x

24528278 Iv Medication Solution Compatibility Chart For Nurses 3g4t66
December 2021 0
Annual Medical Report Form 4mq6s
December 2019 81
Sss Foreclosed For Posting Haa For Sale 1s3w2i
July 2022 0
Advanced ing Chapter 1 1s1311
November 2019 84
Makalah Kewirausahaan r2d4o
January 2021 0